




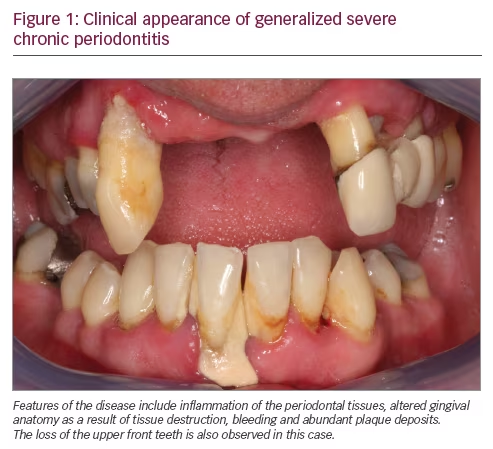
Chronic periodontitis (CP; Figure 1) is a multifactorial inflammatory disease associated with dysbiotic dental plaque biofilms and characterized by progressive destruction of the tooth‐supporting structures.1 CP is a major public health problem due to its high prevalence and because it may lead to tooth loss and disability. CP negatively affects chewing function and thereby nutrition, it is a source of social inequality, and impairs quality of life. Globally, severe CP is the sixth most prevalent disease, affecting 11.2% of the population (95% uncertainty interval: 10.5–12.0%).2 The global cost of lost productivity from severe CP alone has been estimated to be $54 billion per year.3
CP is a non-communicable disease (NCD) that shares social determinants and risk factors with other major NCDs such as heart disease, diabetes, cancer and chronic respiratory disease.4 A bi-directional relationship between diabetes and CP has been recognized for some time,5,6 with the majority of studies focusing on the relationship with type 2 diabetes. The early studies supporting a bi-directional relationship were predominantly cross-sectional in design, precluding the ability to firmly demonstrate direction.7 However, more recent studies including both prospective cohort and interventional studies have provided further insight into the relationship between these two diseases.8
The aim of this narrative review is to summarize recent epidemiological evidence of the relationship between CP and diabetes, and report on the recommendations of a recent joint workshop of the European Federation of Periodontology (EFP) and the International Diabetes Federation (IDF).9
The impact of diabetes on chronic periodontitis
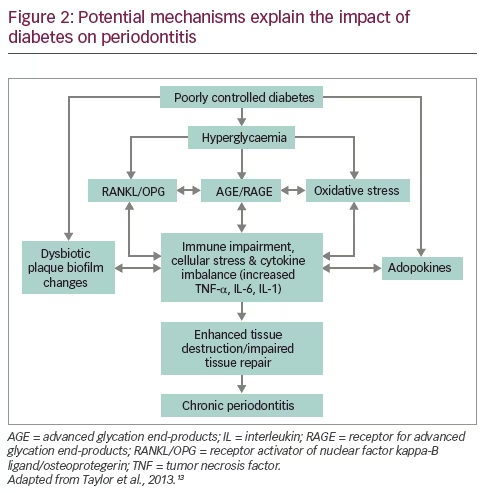
The significance of diabetes as a major risk factor for CP first became apparent in the 1990s in a number of cross-sectional and longitudinal studies investigating the Pima Indian population. The prevalence and incidence of chronic periodontitis was found to be greater in Pima Indians who had type 2 diabetes compared with those who did not.10 It is now well accepted that people with diabetes are more likely to have or develop periodontitis,11 with a threefold higher risk of periodontitis being reported in individuals with diabetes compared to diabetes-free controls.12 Several explanatory mechanistic pathways (Figure 2) have been proposed.13,14 The hyperglycemic state that defines diabetes has several deleterious effects including: the formation of irreversible advanced glycation end-products (AGEs) and the expression of their chief signaling receptor, the receptor for advanced glycation end-products (RAGE);15,16 enhanced levels of reactive oxygen species (ROS) and a state of oxidative stress;17 and modulation of the receptor activator of nuclear factor kappa-B ligand/osteoprotegerin (RANKL/OPG) ratio.18
The irreversible formation of AGEs in particular, can have direct pro‐inflammatory and pro‐oxidant effects on cells.14 When AGEs bind to their signaling receptor RAGE, cellular phenotype and function are critically impacted, and enhanced inflammation, oxidative stress, both of which can further drive AGE formation and impaired tissue repair ensues forming a ‘vicious cycle’. Periodontal infection further potentiates this vicious cycle in the susceptible host with diabetes leading to accelerated and more severe periodontal destruction.
Cumulatively these effects, complemented by dysbiotic dental plaque biofilm changes around the teeth with increased generation of pro-inflammatory cytokines and circulating adipokines resulting from diabetes-associated adiposity and dyslipidaemia, drive a vicious cycle of cellular dysfunction and inflammation. Ultimately, enhanced periodontal tissue destruction and impaired repair ensue, leading to accelerated and severe CP. Factors which are likely to influence these mechanistic pathways include genetics, age, smoking, and stress.
The impact of diabetes on CP was investigated in a population-based study of 2,626 men and women in Germany participating in the Study of Health in Pomerania19 (SHIP). This prospective cohort study aimed to examine the impact of diabetes (type 1 and type 2) and glycemic control on 5-year periodontal status change. Diabetes was determined via physician diagnosis and/or glycated hemoglobin (HbA1c) ≥6.5% (uncontrolled diabetes was defined as HbA1c >7.0%). Both uncontrolled type 1 and type 2 diabetes were associated with increased CP progression and risk of future tooth loss. The authors concluded that it was the level of control of the subject’s diabetes, not the etiology (type 1 or type 2 diabetes), that was the important determining factor for future tooth loss and CP progression.
More recently, 4,033 Taiwanese subjects20 aged 35–44 with no evidence of CP had their fasting plasma glucose (FPG) measured at baseline. In this prospective study the number of newly diagnosed CP cases at re-examination after 5 years of follow-up was n=1,129 (28.0%) in those with normal FPG, 96 (32.3%) in those with pre-diabetes, and n=22 (38.6%) in those with type 2 diabetes at baseline. Multivariable analysis using Cox’s proportional hazard regression model showed an increased risk of incident CP for subjects with pre-diabetes (hazard ratio [HR] = 1.25, 95% confidence interval [CI] 1.00–1.57) and type 2 diabetes (HR = 1.95, 95% CI 1.22–3.13) after adjustment for all known potential confounders. A novel finding of this study was the effect of pre-diabetes on incident CP,20 however, the significance of this finding is unclear as other studies reported that pre-diabetes (and well controlled diabetes) were not associated with CP.21
A recent systematic review addressed whether poorly controlled diabetes was associated with CP onset or progression.22 Thirteen prospective studies comprising 49,262 individuals, including 3,197 with diabetes, met the inclusion criteria. Despite the heterogeneity in the studies a meta-analyses of adjusted estimates showed that diabetes increased the risk of incidence or progression of CP by 86% (RR 1.86, 95% CI 1.3–2.8). There was considerable variability in the case definitions of CP and in the criteria used to define its progression. Further studies are recommended that also take into account an estimate of the cluster effects of common risk factors to help clarify how shared risk factors interact with blood glucose levels to affect the onset and progression of CP.22
Summary
Diabetes (type 1 and type 2) is associated with an increased risk of CP onset and progression, with the level of glycemic control being the important determining factor for future tooth loss and CP progression. Further studies are warranted to assess what effect improved glycemic control has on the progression of CP.8
The impact of chronic periodontitis on diabetes
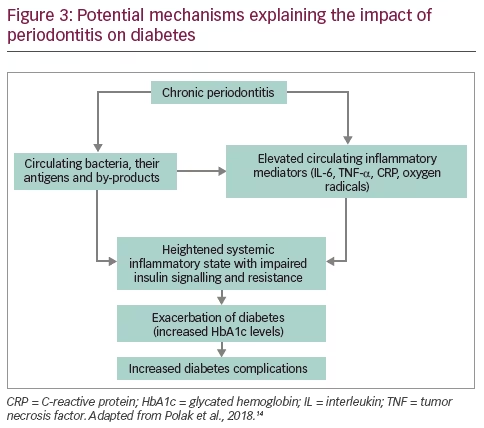
In the reverse direction, CP has the potential to impact the control of diabetes, its associated complications, and also its incidence. From a mechanistic point of view (Figure 3), the evidence supporting the biological plausibility of an impact of CP on diabetes is limited.14 The underlying hypothesis relates to inflammation: CP represents a source of chronic inflammation that contributes to the cumulative systemic inflammatory burden.23,24 The effects of chronic inflammation have been strongly implicated in the development and control of type 2 diabetes.25 Potential key mediators between periodontal inflammation and glucose homeostasis include the cytokines interleukin (IL)-6 and tumor necrosis factor (TNF)-α, the acute phase protein C-reactive protein (CRP) as well as oxygen radicals. All these mediators have been implicated with impaired insulin signaling and resistance.26
Despite the biological plausibility proposed, the complex etiology of both CP and diabetes makes the impact CP has on diabetes difficult to determine from clinical studies. This is largely due to confounding by shared risk factors including age, obesity, sex and some metabolic biomarkers, for both type 2 diabetes27 and periodontitis.28,29 Epidemiological evidence can broadly be divided into studies assessing the impact of CP on glycemic control (in subjects with or without diabetes), the impact of CP on diabetes complications, and the impact of CP on the development of diabetes (type 2).
A number of studies have found that that in diabetes-free subjects, poorer glycemic control (as defined by increased HbA1c, impaired glucose tolerance, or metabolic syndrome prevalence), is exhibited when CP is present.30–32 The impact of CP on insulin resistance, impaired β-cell function, and impaired fasting glucose (IFG) was studied in a cohort (n=19,122) drawn from the from the Korean National Health and Nutrition Examination Survey (KHANES).33 Subjects with CP had a significantly higher prevalence of IFG (28.5% versus 17.7%, p<0.001) and lower homeostatic model assessment-β (115.2 versus 130.8, p<0.001) than those who were periodontally healthy. CP was also quantified as a risk factor for IFG (odds ratio 1.30, 95% CI 1.19–1.42).
A limited number of studies have also assessed the impact of CP on glycemic control in subjects with established diabetes.34 Two large studies found that CP was significantly associated with poorer glycemic control in subjects with type 2 diabetes.35,36 Conversely, two case–control studies did not report a significant difference in HbA1c or fasting blood glucose levels when comparing people with or without periodontitis.37,38
A recent review of 14 studies involving 31,988 subjects concluded that CP in patients with diabetes was associated with a higher presence of diabetes-related complications, including retinopathy, nephropathy, neuropathic foot ulceration, various cardiovascular diseases and death.34
Regarding evidence for the impact of CP on the development (incidence) of type 2 diabetes, a systematic review by Borgnakke et al. identified only four eligible studies.7,32,39–41 The populations studied included a nationally representative sample in the US,39 and three Japanese cohorts.32,40,41 Three of the studies reported that severe CP was associated with the development of type 2 diabetes, after adjustment for various confounders.32,39,41 One study found only a tendency for increased risk.40 A more recent systematic review by Graziani et al. identified a further two studies, both involving Taiwanese cohorts.20,34,42 One study found that over a 5-year period, adults (aged 35–44 years) with evidence of CP presented a 33% increased risk of incident hyperglycemia, including diabetes (adjusted HR 1.33, 95% CI 1.09–1.63) after controlling for potential confounding factors.20 The other study, a larger retrospective study on 44,601 periodontitis-affected individuals, found that type 2 diabetes incidence was higher in patients undergoing periodontal surgical treatment used as a surrogate for severe CP, than in the controls (adjusted HR 1.19, 95% CI 1.10–1.29).42
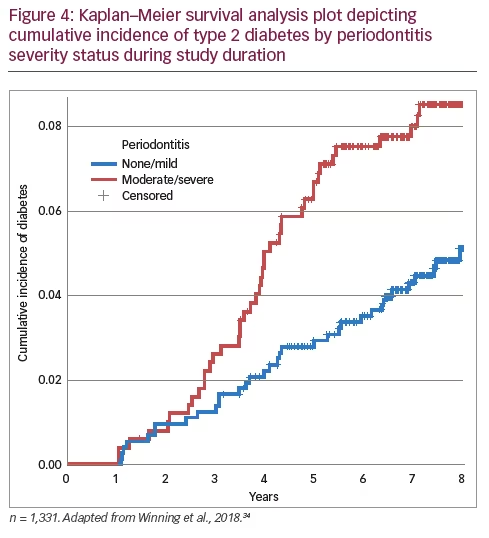
Our own research group, has recently published a prospective longitudinal cohort study aiming to investigate CP as a potential risk factor for incident type 2 diabetes.43 1,338 men without diabetes, aged 58–72 years, in Northern Ireland had a detailed periodontal examination. Parallel to the periodontal examination, participants completed questionnaires gathering information on their medical history, social circumstances, demographic background and tobacco use. A physical examination assessed anthropometric measures including weight and height. Fasting blood samples were obtained and analyzed for total cholesterol level and CRP. There were 80 cases (6.0%) of incident type 2 diabetes during a median follow-up period of 7.8 (interquartile range 6.7–8.3) years. The Kaplan–Meier plot showed that, as time progressed, incident type 2 diabetes probability was significantly greater for men with baseline moderate/severe CP than those with no/mild CP (Figure 4)43. Cox proportional hazards regression analysis showed that men with moderate/severe CP versus those with no/mild CP had an adjusted HR of 1.69 (95% CI 1.06–2.69) for incident type 2 diabetes.
Despite the majority of studies supporting an association between CP and incident diabetes, a recent well-conducted study found no evidence of an association.44 Data from an 11-year follow-up of the SHIP study were analyzed to evaluate the effects of CP on incident diabetes and long-term HbA1c changes in 2,047 subjects aged 20–81 years. Over a mean follow-up period of 11.1 years, 207 subjects developed diabetes. Baseline measures of CP were not significantly associated with either diabetes incidence or long-term changes in HbA1c.44 The conflicting results highlights the need for further studies in different populations.
Summary
Most of the studies examining the impact of CP on diabetes are in relation to type 2 diabetes. In individuals with diabetes, the presence of CP is associated with a deterioration in glycemic control and a higher prevalence of diabetes-related complications. In individuals without diabetes, the presence of CP is associated with poorer glycemic control. CP may potentially be a risk factor for the development of type 2 diabetes in individuals without diabetes.
Interventional studies
The United Kingdom Prospective Diabetes Study (UKPDS) and the Diabetes Control and Complications trial in the US have demonstrated that intensive treatment of hyperglycemia can reduce the risk of long-term diabetes complications.45–47 A 1% reduction in the HbA1c in the UKPDS was associated with a relative risk reduction of 21% for any diabetes-related endpoint, 21% for diabetes-related deaths, 14% for myocardial infarction and 37% for microvascular complications.46 Since CP has been associated with poorer glycemic control, an important question is whether periodontal treatment could be an effective therapy to improve glycemic control.
Treatment of CP is carried out non-pharmacologically and normally involves the provision of oral hygiene instruction aimed at educating and motivating the patient to address the cause of their CP, mainly the buildup of plaque bacteria around the teeth. Additionally to this, mechanical debridement (scaling and root planing) by a dentist, periodontist, or hygienist is often required to remove both plaque and plaque deposits that have mineralized and hardened (calculus). More advanced forms of the CP may necessitate a surgical approach to disease management.
A recent Cochrane systematic review that investigated the effect of periodontal therapy on glycemic control of people with diabetes48 included 35 parallel randomized controlled trials comprising 2,565 participants. The majority of studies (33; 94%) targeted patients with type 2 diabetes. Low quality evidence from 14 studies (1,499 participants) comparing periodontal therapy with no active intervention/usual care demonstrated that mean HbA1c was 0.29% lower (95% CI 0.10%–0.48%) 3–4 months post-treatment. This is broadly the order of magnitude expected by adding a second oral antidiabetic medication.49 Only five studies extend beyond 3 months follow-up. In these studies, periodontal therapy was associated with a 0.02% lowering of HbA1c after 6 months, however, it was not clear whether this was significant, as the 95% CI ranged from 0.20% lower to 0.16% higher.
A recent study investigated the effect of periodontal therapy on glycemic control in people with type 2 diabetes with a 12 month follow-up.50 264 patients with type 2 diabetes were randomly assigned to either receive ‘intensive’ periodontal treatment (including periodontal surgery where appropriate), or control periodontal treatment. Treatment allocation included a process of minimization in terms of diabetes onset, smoking status, sex, and periodontitis severity. The primary outcome was between-group difference in HbA1c at 12 months in the intention-to-treat population. At baseline, mean HbA1c was 8.1% (standard deviation [SD] 1.7) in both groups. After 12 months, unadjusted mean HbA1c was 8.3% in the control group and 7.8% in the intensive treatment group; with adjustment for baseline HbA1c, age, sex, ethnicity, smoking status, duration of diabetes, and body mass index, HbA1c was 0.6% (95% CI 0.3–0.9; p<0.0001) lower in the intensive treatment group than in the control group.50
Despite the majority of clinical trials supporting a hypothesis that successful periodontal treatment improves glycemic control in individuals with type 2 diabetes, a lack of consensus remains. Indeed, a number of studies have found that periodontal treatment has no effect on glycemic control.51–54 In 2013, Engebretson and colleagues reported the results of a large multicenter clinical trial investigating the effects of periodontal treatment on HbA1c levels with 6 months follow-up.53 514 patients were enrolled across five centers. As the trial progressed, enrollment was stopped early because of futility. At 6 months, mean HbA1c levels in the periodontal treatment group increased 0.17% (SD 1.0), compared with 0.11% (SD 1.0) in the control group, with no significant difference between groups based on a linear regression model adjusting for clinical site (mean difference –0.05%, 95% CI –0.23–0.12; p=0.55).
The controversy regarding the effect of periodontal treatment on glycemic control may be the result of several issues relating to trial design including: uncertainty over what constitutes successful periodontal treatment; variability in baseline levels of glycated hemoglobin; and variable follow-up times.55 Ultimately, this highlights the need for further well-designed studies.
Summary
Evidence from the literature suggests that successful periodontal treatment, which results in the reduction in inflammation from the periodontal tissues, may have the potential to improve the metabolic control of people with diabetes.56 However, further studies are required to provide more conclusive evidence.
The European Federation of Periodontology and the International Diabetes Federation Workshop 2017
Experts from the fields of gum health and diabetes met for a ‘Perio-Diabetes Workshop’ in 2017, the outcomes which have recently been published.9,14,34,56 The aim was to examine the latest evidence linking periodontal diseases and diabetes. Among the key conclusions reached were:
- there is strong evidence that people with CP have elevated risk for dysglycaemia and insulin resistance;
- there is a moderate level of evidence that certain biological mechanisms mediate the effect of CP on the control of diabetes;
- patients with CP have a higher chance of developing type 2 diabetes; and
- there is evidence that improving periodontal health has benefits in improving metabolic control and/or the complications of diabetes.
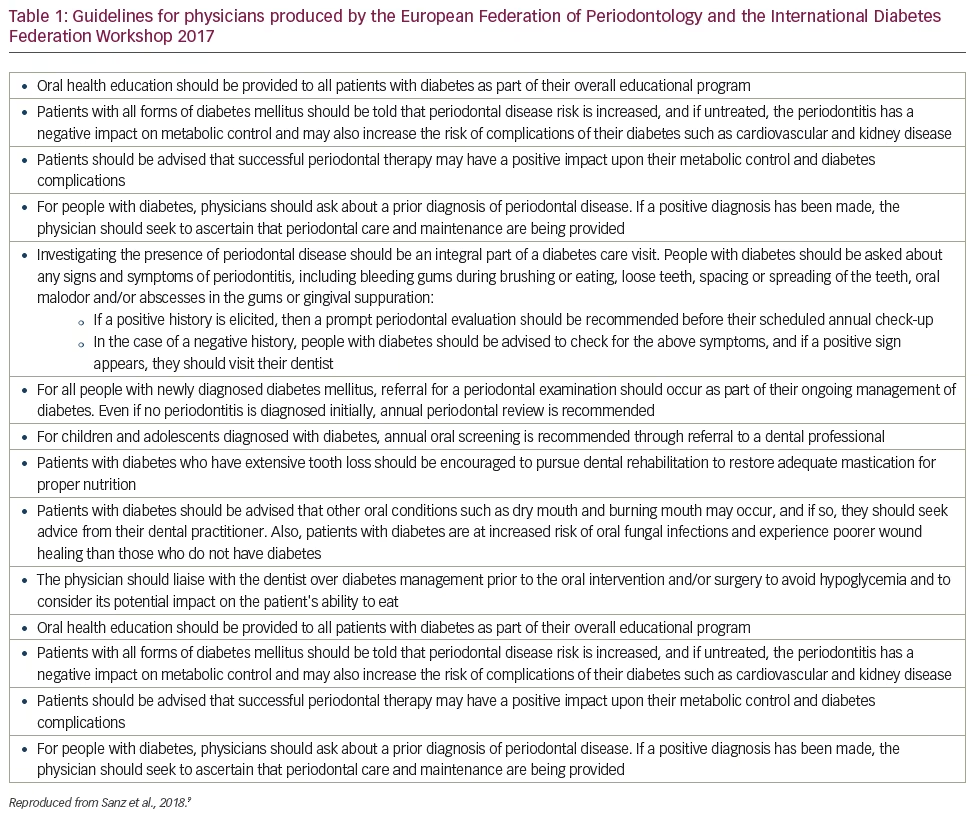
A number of management guidelines for physicians, oral health professionals, and patients were proposed. In particular, because of the increased risk for developing periodontitis in patients with diabetes and the negative impact of periodontitis on diabetes control and complications, specific recommendations to physicians were published (Table 1).9
Conclusions
A growing body of evidence is beginning to unravel the complex relationship that CP shares with diabetes. The biological rationale connecting CP and diabetes relates to the common theme of chronic inflammation. Diabetes (type 1 and type 2) is associated with an increased risk of CP onset and progression, with the level of glycemic control being the important determining factor for future tooth loss and CP progression. In the reverse direction, evidence has emerged that CP may adversely affect glycemic control in both diabetic and non-diabetic subjects. In subjects with diabetes, there is a direct and dose-dependent relationship between periodontitis severity and diabetes complications.11 CP may also associated with an increased risk of incident type 2 diabetes. Periodontal therapy is safe and effective in people with diabetes and may be associated with short term reductions in HbA1C. Whilst further studies are needed, the available evidence does highlight the importance of good oral health in relation to systemic health.


