




India has a vast diversity of cultures and religions following a vast number of festivals and rituals irrespective of their caste, creed, age, and status with different rituals.1 The Hindu religion constitutes the world’s third largest religion and 80% of the Hindu population resides in India and Nepal.2 According to the All India Religion Census Data 2011, Hindu religion comprises 79.80%, Muslim 14.23%, Christian 2.30%, Sikh 1.72%, Buddhist 0.70%, Jain 0.37%, and others 0.66%.3 Many types of fasts are observed by different religions as a ritual meant to purify the body and the mind, and develop the sattvic quality of detachment as a mark of respect to personal gods, or as a part of penance.4,5 In the healthy subject, fasting does not have any harmful consequences on health. However, it can induce dehydration, dyselectrolytemia, hypotension, hypoglycemia, and significant hyperglycemia for patients with diabetes.6,7 Data regarding religious fasts in subjects with diabetes are primarily available in the context of Ramadan fasting.8–10 To the best of our knowledge, there is no data regarding dietary practices during fasts in subjects with type 2 diabetes mellitus (T2DM) among the Hindu religion from India or any other country.
Navratri and Karvachauth among Hindus, and Ramadan among Muslims are the most common religious fasts observed in India. Navratri is one of the most widely celebrated festivals by Hindus in India. It is a 9-day festival devoted to the worship of goddess Durga. The people observe fasts, worship the goddess (northern India), perform “garba” and “dandiya-raas” dances (western India), and follow unique tradition-bound activities in different states with different cultural beliefs.4 Similarly, during Karvachauth, Hindu women observe a long day fast for about 12–15 hours, usually without even consuming water, and pray for their husband’s long-life good health.6
Fasting during diabetes can cause changes in diet and physical activity.7–10 In general, under controlled circumstances, intermittent fasting has shown to be beneficial to improve glucose homeostasis, insulin resistance, weight loss, and cardioprotection.11 However, it may throw off the delicate balance of food, water, and blood glucose levels in potentially harmful ways increasing the risk of hypoglycemia, ketoacidosis, as well as thrombotic complications.6,8–13 A sudden change in dietary habits can cause harmful and unmanageable impacts on blood glucose levels causing short- and long-term complications.13–17
The main objective of the study was to assess the dietary practices of people with T2DM during fasting with a special focus on the common Hindu fasts: Navratri and Karvachauth. We also aimed to identify the eating patterns and nutritional assessment during fasting in subjects with T2DM among different religions in North India.
Methods and participants
This was a retrospective, cross-sectional, non-interventional, questionnaire-based study performed in the outpatient department of three diabetes clinics in northern India (two from Delhi/NCR and one from Bhopal). Patients who consented were subjected to predesigned proforma. Exclusion criteria included people with diabetes other than T2DM, those suffering from any major disease and who were unwilling to participate.
Data were collected using a structured, multiple-choice, questionnaire that contained sections on socio-demographic profile (age, religion, monthly income, marital status, household type [nuclear/joint], and educational qualification), anthropometric assessments, medical therapy, and information on dietary and self-care practices during fasts. Among dietary practices, we specifically focused on collecting data related to food groups, with type of food items allowed, frequency of eating and general cooking methods used during the period of fasts. The two most common Hindu fasts (Navratri and Karvachauth) were studied in detail. Both English and Hindi proforma were used as per each participant’s preference. Hindi translation was done with the help and validation by two language experts. The questionnaire was pilot tested on 30 subjects, who were not included in the study. Data were collected during the period of January–March, 2018.
Statistical analysis
Data were entered and consolidated in Microsoft Excel 2010 version. Categorical variables were presented in number and percentage, and continuous variables were presented as mean ± standard deviation. The analysis was done using Statistical Package for Social Sciences (SPSS; Chicago, Illinois, USA) version 21.0 software.
Results
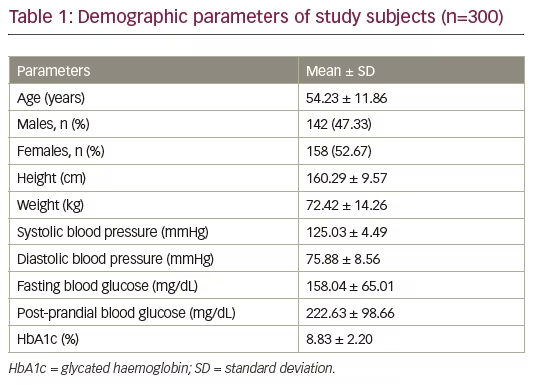
A total of 300 subjects participated in the study (age 54.23 ± 11.86 years). The demographic and glycemic parameters of study participants are shown in Table 1. The average time taken to complete the questionnaire was 15–20 minutes. Regarding pharmacotherapy, 93.33% of study subjects were taking metformin, 57.00% were on sulfonylureas, and 30.33% of subjects were on insulins along with oral anti-diabetic medications. All subjects were receiving at least one drug for the management of hyperglycemia. Regarding complications, 19.66% of participants had peripheral neuropathy, 13.33% had nephropathy, 5.00% had retinopathy while known coronary artery disease was present in 8.33% of subjects.
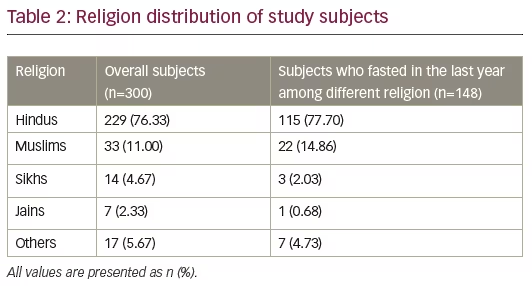
The distribution of study participants with respect to their religion and practice of fast are shown in Table 2. The subjects were dominantly Hindus (76.33%), followed by Muslims (11.00%). The remaining 12.67% participants were Sikh, Jain, and from other religions. Overall, 148 (49.33%) participants observed at least one fast in the last year (2017–2018). Among the participants who observed fasts, 77.70% were Hindu, 14.86% were Muslim, 2.03% were Sikh, 0.68% were Jain, and 4.73% were from other religions (Christian and Buddhist).
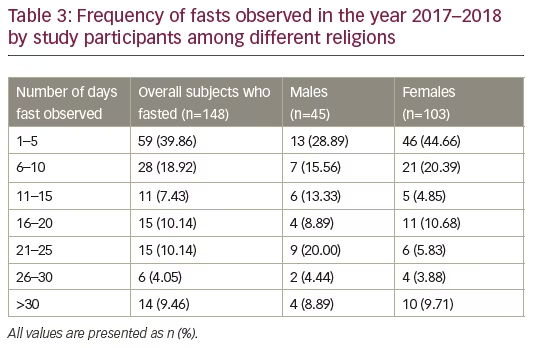
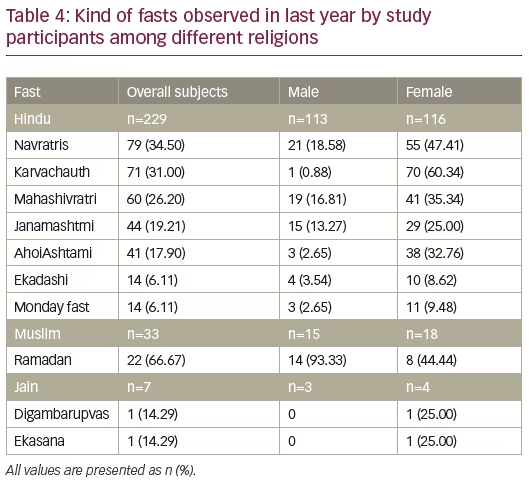
Out of subjects who observed fasts (n=148), 59 (39.86%) patients observed 1–5 days of fasting, 28 (18.92%) observed 6–10 days of fasting, and 14 (9.46%) fasted for >30 days in past year (Table 3). Among Hindus, the most commonly observed fasts were Navratris (by 18.58% of males and 47.41% of females) and Karvachauth (0.88% of males 60.34% of females). Among Muslims, Ramadan was the most common fast (66.67%), and among Jains, Digambarupvas and Ekasana (14.29% each) were common fasts (Table 4).
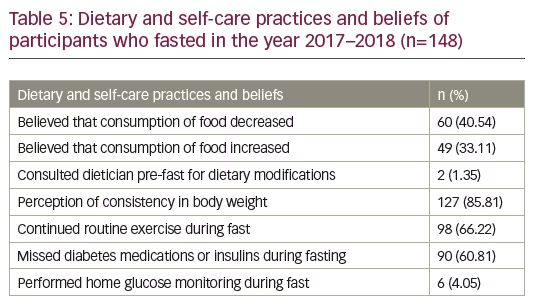
The common dietary and self-care practices followed during fasting are shown in Table 5. Out of all the participants, 40.54% had the perception that their calorie consumption decreased, and 33.11% thought their calorie consumption increased during the period of fasting. Only 1.35% of participants consulted their dietician for pre-assessment and dietary modifications. The majority of the patients (85.81%) believed that their weight remained neutral (72.42 ± 14.26 kg [this is an estimation of weight; as this was a retrospective study, exact weight was not measured at baseline]) during fasting. Despite the fact that the majority of patients (57.00%) monitored blood glucose, only 4.05% actually checked their glucose levels during their last fast. The majority of the patients (66.22%) continued their exercise routine during periods of fast.
The detailed dietary practices followed during the most common Hindu fasts (Navratri and Karvachauth) were explored further. As summarized in Table 6, 65.82% participants reported that they ate three times a day (one meal with two small snacks, such as fruits or tea) during Navratri. During Navratri and Karvachauth fasts, 15.19% and 49.30% of participants, respectively, ate only once a day (one meal with no snack), while 18.99% and 35.21% ate twice a day (one meal with one snack). Most of the participants reported that they ate home-made items instead of readymade outside food and packet items during Navratri and Karvachauth (98.73% and 95.77% of participants, respectively). Milk and milk products, fruits and cereals (especially potatoes) were the most commonly reported food groups consumed, besides pulses, meat and meat products. The preferred cereals during Navratri were buckwheat flour (38.27%), amaranth flour (9.34%), water chestnut flour (26.12%) and barnyard millet (20.13%); while during Karvachauth, wheat flour was consumed by 45.60%. Only 2.62% consumed other cereals in Karvachauth. Direct intake of sugar in the form of sweets/desserts as well as sugar-containing beverages, juices, and soft drinks was also very common, while pulses were the food group that was least eaten.
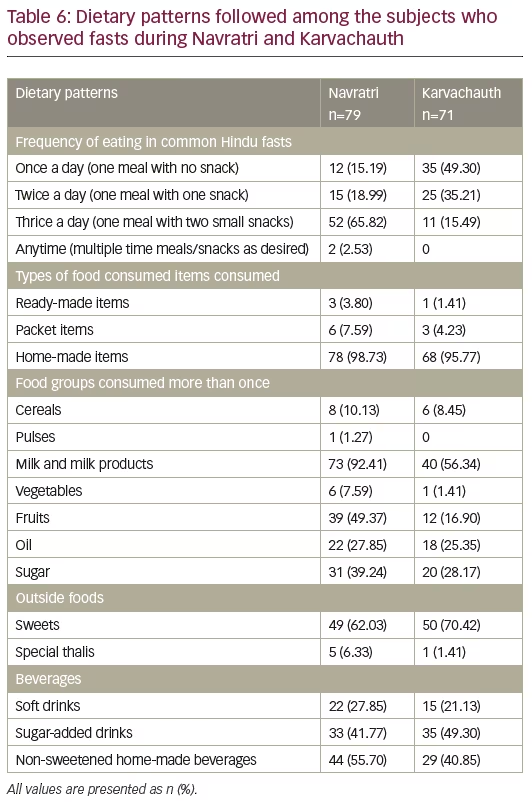
Among participants who observed Navratri, 47.64% consumed food prepared by frying (shallow or deep frying); 62.03% consumed sweets, Indian desserts (Rasmallai, kheer, sweet rice, rasgulla, barfi, kalakand), and jaggery; 41.77% consumed sugar-added beverages (tea, lime soda, milk, butter-milk, shakes); and 27.85% consumed soft drinks. Among participants who observed Karvachauth, 38.90% consumed food prepared by frying (shallow or deep frying); 70.42% consumed sweets, Indian desserts (like Barfi, rasmallai, kheer, rasgulla), and jaggery; 49.30% consumed sugar-added beverages; and 21.13% consumed soft drinks.
Discussion
This cross-sectional study was conducted to assess the dietary and selfcare practices during religious fasts in people with T2DM from northern India, with more focus on the common Hindu fasts. Our study found that fasting practices are common in subjects with T2DM from all religions. The most common Hindu fasts were Navratri and Karvachauth. Navratri was observed commonly among both genders while Karvachauth was found to be predominantly observed among women. This showed that Hindu females, overall, tend to observe more fasts as compared to Hindu males. The study also showed significant erratic dietary practices during days of fasts. This signifies the need to educate people with T2DM, and improve self-care practices among them and their families.
Exploring dietary practices during fasts, it was seen that the frequency of eating during fasts varied among different religions, as well as type of fast. Most of the participants reported eating three times a day (one meal with two small snacks) during fasts. The composition of that meal is reflected to be high in glycemic load which may elevate post-prandial blood glucose levels. The recommended pattern of 5–6 meals (3+3 meal pattern), with respect to the compliance for medical treatment for the achievement of optimum glycemic control, was not followed by any patient during fasting. In our study, only two (1.35%) participants consulted their doctor/dietician for pre-assessment and dietary modifications. The literature on Ramadan fasting has also similarly reported erratic meal patterns, medical ignorance, and deteriorating glycemic control among the people with diabetes.14–20 A study conducted by Al-Arouj et al. in 2010, highlighted general considerations on individualization, frequent monitoring of glycemia, nutrition, and exercise, for the management of diabetes during Ramadan.21
The food groups most consumed during Navratri and Karvachauth fasts were milk and milk products, fruits and cereals. Fats and sugars were also reported to be significantly consumed. As a part of medical nutrition therapy for optimal glycemic control and prevention of complications, it is advised to include an adequate proportion of food groups to meet the dietary recommendations of nutrients. Dietary recommendations for food groups and macronutrients for people with diabetes have previously been defined.21 Regarding food groups, half the food plate should consist of fruits and vegetables, while the other half is divided between whole grains or flour of low glycemic index and lean sources of protein with carbohydrate distribution and adequate intake of non-fat or low-fat dairy source throughout the day. These principles remain similar even during the period of fasts. However, the participants in the present study displayed erratic food-group consumption, carbohydrate distribution, and glycemic load of the meals during fasts. The intake of certain food groups, i.e., cereals, pulses and vegetables, was inadequate, while the intake of fats and sugars was much higher than recommended. In our study we specifically studied flours used during the period of fasts as this is the most important source of carbohydrate for most Indians. Wheat flour is the most commonly consumed flour in non-fasting days among Indians. The flours consumed during fasting days had similar glycemic index to that of wheat flour.
In our study this change in food groups is likely to cause significant changes in blood-glucose levels, which is likely to be compounded by inconsistencies in the amount eaten and the timing of meals. Additionally, this pattern is unlikely to meet the nutritional needs of these individuals.4 A study published by Zainudin et al. in 2017 on Ramadan fasting in people with diabetes, also showed that patients had misconceptions about food groups and impacts of different food groups on blood glucose levels.22
The most common cooking method was frying (shallow and deep frying) with significant usage of direct sugar sources, which is likely to result in making the meal more calorie-dense disturbing the post-prandial blood glucose levels. In contrast to the findings of Yaacob et al., direct intake of sugar in the form of sweets/desserts, as well as sugar-containing beverages, juices and soft drinks, was very common in our study.19 Hence, dietary pattern showed imbalance in the nutritional compositions and erratic meal patterns followed during fasts. The judicious practice of basic dietary recommendations can be easily followed during fasting and feasting given fast-specific counselling.4,6,23–25
To the best of our knowledge, this is the first study to focus on practices during fasts in people with T2DM among Hindus, in northern India. There were several limitations of this study which should be noted. This was a cross-sectional study based on retrospective questionnaire-based information. The study involved a volunteer group which limits generalizability. Religion-based as well as gender-based sub-group analysis was limited by small number of patients. Also, data on calorie consumption using detailed methodology could not be collected.
Conclusion
Erratic dietary practices are common during fasting among subjects with T2DM among Hindu religion in northern India. The majority of participants in this study did not discuss their fasting habits with their diabetes care team. Diabetes care teams should discuss fasts with their patients with T2DM. They should tailor this information based on the patient’s religion and provide them with information regarding diet during days of fast.


