Obesity, defined as the presence of excess body fat, is a major public health problem which appears to have become endemic to the human race.1 Owing to its multifactorial etiopathogenesis, clinical manifestations and comorbidities, the management of obesity can be more challenging than that of other chronic medical conditions. Although there has been much debate surrounding whether obesity is a disease in itself, or just a contributor to other diseases, obesity does fit the criteria for disease definition and thus has been officially recognised as such by several medical associations, societies and international health organisations.2 The definition and classification of obesity has not been standardised; the criteria used differs according to the geographical location and ethnicity of the patient.3 In addition, the utility of body mass index (BMI) in diagnosing obesity is not an infallible means of assessment.4 The recognition of obesity in patients classified as being of ‘normal weight’ according their BMI, highlights the shortcomings of the measure.5
There is much more to obesity than just a number; the metabolic, musculoskeletal, and psychological functioning associated with body weight all contribute to the impact of obesity on health and quality of life.6 Even those with normal weight who demonstrate cardio-metabolic obesity associations are at greater risk of mortality compared to those who may be obese as defined by their BMI, but have normal metabolic health.7 Patients who fit within the latter category, who do not show metabolic abnormalities such as hypertension, dyslipidaemia, and dysglycaemia, are often referred to as being ‘metabolically healthy obese’ (MHO).8,9 Several meta-analyses have previously confirmed a positive association between an MHO phenotype and the risk of cardiovascular events, although the precise definition of MHO is yet to be described.8,9
When it comes to treating obesity, modern bariatrics sometimes confuses, rather than clarifies, clinical decision making, and treatment is often associated with unsatisfactory outcomes for those living with obesity, as well as their health care providers.10 Various fad diets, behavioural therapies, unproven medical treatments and aggressive surgical ‘cures’, along with their often-exorbitant expense, all compete for a place in the expanding portfolio of promoted ‘quick-fix’ treatments. The proliferation of such approaches contributes to the confusion surrounding obesity care.10
Person-centred care
Chronic disease management, based upon the biopsychosocial model of health, encompasses the importance of person-centred care. Though person-centred care is followed in various endocrine and metabolic conditions, such as diabetes, hypothyroidism and menopause, its relevance is not highlighted in obesity. The relatively few articles on the person-centred management of obesity focus on the psychosocial aspect of nursing and are limited to case reports or series.11,12
In this editorial, we propose a robust framework to facilitate the use of person-centred techniques and tools, as well as targets and therapies, in obesity. Each person living with obesity is different, thus obesity management should be individualised. Through this discussion, we hope to focus the attention on person-specific needs and to help healthcare providers craft appropriate strategies that are able to fulfil these needs.
Techniques
Person-centred obesity care begins with screening and diagnosis. Conventionally, BMI has been used to evaluate obesity, with ethno-specific value cut-offs for Asia-Pacific populations as proposed by The World Health Organization.3,13 These cut-offs, which are lower than those for Caucasians, reflect a higher risk of metabolic complications at lower BMI levels in this ethnic group. In spite of using these criteria, there is a subset of people with normal weight obesity that can be identified only by measuring body fat composition.4 There may be people who are more concerned about waist circumference, or waist hip ratio, rather than overall weight or BMI.2 It is imperative, therefore, to develop more accurate means of diagnosing obesity. Until this is done, multiple anthropometric and non-invasive markers, including waist circumference and body fat percentage, may be used to ensure person-centric diagnosis.
The ‘4M’ approach
Screening should not be limited to anthropometry alone as obesity can impact the body in various ways. The ‘4M’ approach advocated by Canadian Obesity Association differentiates between metabolic and mechanical (musculoskeletal) dysfunction, and highlights the deleterious impact of weight on financial health. The four ‘M’s are: metabolic, mental, mechanical and monetary factors. The influence of these factors on health varies not only from person to person, but also from time to time and this must be taken into account when planning treatment.14
The Edmonton Obesity Staging System
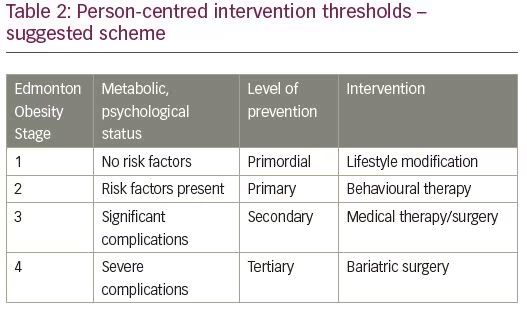
The Edmonton Obesity Staging System (EOSS) provides a rational and pragmatic means of assessing individuals with obesity. The EOSS grades obesity into Stages 0–4. Stage 0 is indicated in persons with No apparent risk factors, physical symptoms, psychopathology, functional limitations and/or impact on well-being related to obesity. Stage 1 implies the presence of obesity-related subclinical risk factors, and mild physical symptoms, psychopathology, functional limitations and/or impairment of well-being. Stage 2 obesity is defined if established vascular-metabolic and/or psychological obesity-related dysfunction are noted. Stage 3 obesity suggests the presence of end-organ damage (such as myocardial infarction, heart failure, stroke, significant psychopathology, etc.) and Stage 4 obesity suggests severe, potentially end-stage, obesity-related disabilities.15
EOSS enables a holistic approach to obesity, viewing the person not only through a numerical prism that focuses on weight and waist measurements, but as a whole being, with physical, mental and emotional needs. EOSS highlights both biomedical and psychological aspects of obesity, thus acknowledging the biopsychosocial model of health.
The SECURED model
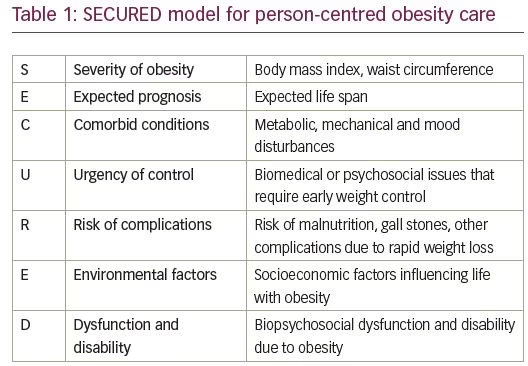
We propose the SECURED (Severity of obesity, Expected prognosis, Comorbid conditions, Urgency of control, Risk of complications, Environmental factors, Dysfunction & disability) model to manage obesity in a holistic manner. The SECURED model includes a seven-pronged evaluation of weight and its complications, and helps plan an individualised approach to therapy (Table 1). Individuals experiencing severe conditions comorbid to obesity, a high level of dysfunction/disability and/or an urgent need for treatment (e.g., the presence of a life- or organ-threatening complication) justify aggressive management. In contrast, if the expected benefit/lifespan outcome for a patient is poor, if there is a risk of iatrogenic complications, and/or if there are other environmental factors at play, a more cautious approach to treatment may be warranted.
SECURED is similar in philosophy to EOSS, but it does not try to split patients into separate artificial compartments. As well as the conventional biomedical aspects of obesity, the SECURED approach includes environmental and iatrogenic factors as important aspects to be considered in the management of obesity. The SECURED model encourages the treating physician to perform a risk/benefit analysis prior to planning any intervention and thus acts as an aid to clinical decision making, rather than as a mere classification rubric.
Thresholds and tools
Neither EOSS nor SECURED suggest specific thresholds for diagnosis, therapy initiation, or therapy intensification (Table 2). Using EOSS as a basic framework, however, we suggest the following: EOSS Stages 0 and 1 are targets for primordial and primary prevention, which are best achieved by lifestyle modification and behavioural therapy. EOSS Stage 2 requires secondary prevention, which can be offered through meal replacement and medical weight loss therapies. For EOSS Stages 3 and 4, tertiary prevention is needed. Along with behavioural and medical intervention, bariatric surgery may be required. It must be noted that this suggestion needs to be interpreted by the healthcare provider in the context of the individual patient.15,16 It is also noteworthy that management of any comorbid metabolic, mechanical and mood disorders should continue concurrently and this is often best done in a multi-disciplinary clinic setting.17
Targets
The targets for obesity management should be as person-centred as any proposed treatment. The aim of weight loss is not just to achieve an ideal number. An ideal weight or waist circumference should not represent an end-goal, instead, it is a means of attaining a eumetabolic, eufunctional, euthymic state. In this regard, our suggested model for setting targets, the ‘BaroSixer’ model (Figure 1), mirrors the WHO’s sempiternal definition of health. This hexad, which is similar to existing models in diabetes care, is based upon the game of cricket, in which a ‘sixer’ represents the highest score possible with a single ball.
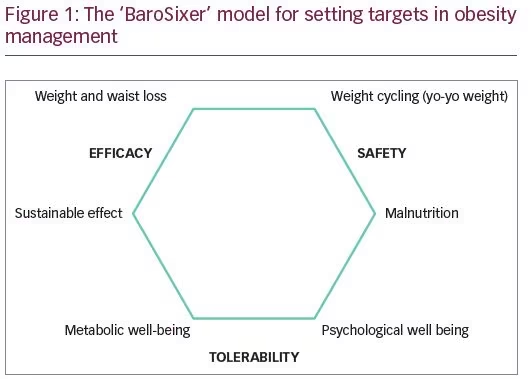
The BaroSixer lists six arms of therapy, of these, two are related to efficacy (best achievable weight, best achievable waist circumference), two to safety (avoidance of yo-yo weight pattern/weight cycling and avoidance of malnutrition) and two to tolerability (metabolic wellbeing and psychological wellbeing). Whatever the tools used, our aim should be to score a ‘sixer’ for each person living with obesity. It is important to carry out a realistic assessment of achievable goals; the maximum possible healthy weight loss must be discussed and agreed with the patient, and documented.
Though several guidelines have been published by national and international bodies for the clinical management of obesity, only a few of them emphasise patient-centric management.18–20 A recently published paper by the European Association for the Study of Obesity (EASO) provides a comprehensive algorithm for the personalised management of obesity, for general practitioners.21 Models such as SECURED and BaroSixer would help in the simple and inclusive implementation of such guidelines. Evidence on the utility and impact of using similar structured models is provided from the long term follow-up data following EOSS staging.16
Summary
To summarise, we propose a simplified yet comprehensive approach for the evaluation and management of obesity. The SECURED and the BaroSixer models offer value in managing obese individuals, and may help improve patient satisfaction as well as outcomes. These models should also serve as useful learning tools for obesity care providers of all disciplines.