Abnormal eating behaviors involve deliberately adjusting food intake to the point of it being insufficient or excessive, which tends to harm the physical and mental health of an individual.1 The concern often exists amongst students regarding their body image, specifically around being overweight and obese. This ideology may be influenced by societal pressures as a slim body is widely considered to be physically attractive.2,3 An expansive range of techniques to lose weight have been promoted to capitalize on this mindset, including hypocaloric diets, restrictive eating habits, nutritional compounds, pharmaceutical products, and extreme measures to reduce calorie intake, such as skipping meals entirely.4–6 Studies have shown clear associations between the perception of body weight, body image, and the appearance of disturbed eating behaviors among undergraduate universities’ students. 2,3,6,7 The body mass index (BMI) is an anthropometric tool calculated using the height and weight of an individual. It is an easy screening method to identify those who are overweight or obese and thus at greater risk of health problems.
Abnormal eating behaviors are challenging to detect since an individual exhibiting them may not display any obvious signs. An individual who has an abnormal eating behavior may experience physical and mental stress.1,3,5 Adolescents who engage in abnormal eating behaviors are often unaware of the detrimental effects of such behaviors on mental and physical health. This lack of awareness may worsen their health due to the delay in seeking medical advice and leaving the disorder untreated.4,5 This may then cause negative consequences, including increased mortality rate, as shown in anorexia.4,5 In Malaysia, a person’s eating behaviors are rarely assessed. If any abnormal eating behaviors do happen to be identified, addressing them is unlikely to be considered a priority in patient management.8 However, there is evidence to suggest that Malaysians do fear being overweight and desire to be thinner, even when they are classed as having a normal body weight.6,8
Enrolling at university often involves a significant change in lifestyle to accommodate study requirements. These changes, coupled with the stresses associated with university life, can put university students at risk of developing abnormal eating behaviors and of becoming overweight or obese, which may significantly impact their health and quality of life.8–10 Stress levels may increase as students advance through their studies and are faced with more challenges, greater demands, and increasing responsibilities, which can lead to feelings of insecurity, poor sleep, anxiety, and depression, which can cause and heighten risk for abnormal eating behaviors.8–10 Determining the prevalence of abnormal eating behaviors in university students and the association between these behaviors and BMI will help authorities, commanding institutions, and researchers to take effective measures to reduce their potentially detrimental effects. The principal aims of the present study were to determine the prevalence of abnormal eating behaviors among students of the Malaysian Allied Health Sciences Academy (MAHSA) University and to explore whether abnormal eating behaviors are associated with BMI, waist circumference, waist-to-height ratio and/or gender.
Methods
Research design
A descriptive cross-sectional study was conducted among MAHSA University students from March to May 2019 with the following aims: (1) to determine the association of abnormal eating behaviors with BMI, (2) to determine the prevalence of abnormal eating behaviors, and (3) to determine the demographic and anthropometric characteristics of the students with abnormal eating behaviors.
Participants
The target population comprised students enrolled at MAHSA University in Malaysia studying a range of different academic disciplines. A convenient sample of 300 participants was included in this study.
Data collection
Students who agreed to participate in the study were given a set of questionnaires that included a participant information sheet outlining the objectives of the study, study design, methodology, expected outcome, significance of the study, and a statement confirming confidentiality of the collected data , a consent form, a socio-demographic questionnaire, and the Eating Attitude Test 26 (EAT-26) questionnaire. A total of 300 copies of the self-administered questionnaire sets were distributed among students with a 100% response rate. Anthropometric measurements including height, weight, and waist circumference were taken. Using the obtained measurements, the BMI of the respondents was calculated as weight divided by height squared (kg/m2). Waist-to-height ratio was also calculated.
Socio-demographic questionnaire
The socio-demographic questionnaire included information about the demographic characteristics of the students such as their age, gender, university course they study, year of study, and faculty.
Body mass index
The BMI calculation was based upon the BMI chart as suggested by the World Health Organization (WHO). According to the Asian Pacific WHO cut-off points, a BMI score of <18.5 kg/m2 is considered underweight, a BMI of 18.5−24.9 kg/m2 is classed as normal weight, a BMI of 25−29.9 kg/m2 is considered overweight, and a BMI score of ≥30 kg/m2 indicates obesity.11
The Eating Attitude Test 26
The EAT-26 tool (English version) was used to screen for eating-disorder characteristics and behaviors among students. The EAT-26 is widely used and was designed to provide a standardized measure of symptoms and characteristics of abnormal eating behaviors.12 The validity and reliability of the scale items showed internal consistency, and a Cronbach’s alpha of 0.82.
The EAT-26 consists of 26 items. Each item (except the 25th item) has six response options ranging in value from 0 to 3 (“always” = 3; “almost always” = 2; “often” = 1; and “seldom”, “hardly ever”, and “never” = 0). Item 25 has a reversed score (“always”, “nearly always” and “often” = 0; “seldom” = 1; “almost never” = 2; and “never” = 3). The total score of EAT-26 equals the sum of scores for the 26 items. A score of ≥ 20 is defined as being characteristic of a “disordered eating attitude”. The EAT-26 questionnaire also includes five behavioral questions that are used to assist in determining eating behavior over the past 6 months, given before answering the questionnaire. These questions investigate eating “binges”, defined as eating much more than most people would under the same circumstances and the feeling that eating is out of control. It also includes questions to investigate whether a person has made themselves sick (self-induced vomiting) or used laxatives, diet pills, or diuretics to assist in controlling their weight. The behavioral questions investigated whether a person exercised for more than 60 minutes per day to lose or to control his/her weight and whether there had been a weight loss of 10 kg or more in the past 6 months.12
Data analysis
Data entry and analysis were performed utilizing the Statistical Package for the Social Sciences (SPSS), Version 24. Basic descriptive statistics were run for all variables to establish means and standard deviations for variables measured on continuous scales, and frequencies and percentages for categorically measured variables. Correlation analysis was conducted to examine the association between eating behaviors and the BMI of the study participants and an independent t-test was used to determine the association between abnormal eating behaviors and gender; p<0.05 indicates a significant result.
Ethical considerations
The ethics committee of MAHSA University approved the study (approval number: RMC/EC50/2019). Participants signed an informed consent form after the purpose of the study had been explained and were assured about the confidentiality of their responses.
Results
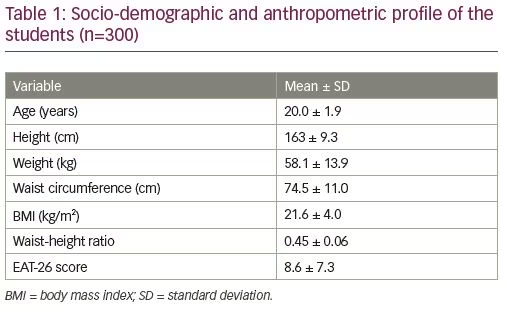
A total of 300 students participated in the study. Among 300 respondents, 193 respondents (64.3%) were female and 107 respondents (35.7%) were male. Most of the students (67.7%) were 20−30 years of age, 36.3% were aged <20 years, and the mean age of the study population was 20.3 ± 1.90 years. Of the students who participated, 30.3% were from the school of medicine, 20.7% were undertaking pre-university studies, 17.0% were studying health and sport sciences, and 12.7% were from the faculty of dentistry. The remaining 19.3% were from other faculties, including nursing, engineering, pharmacy, and business, financial, and hospitality.
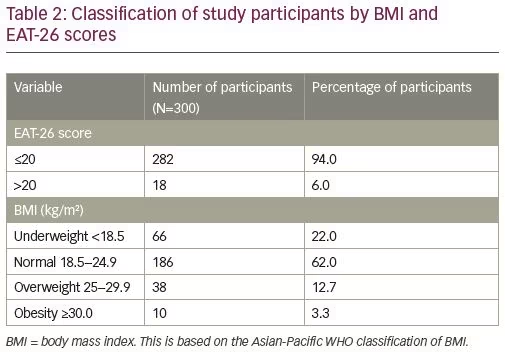
The mean BMI was 21.6 ± 4.03 kg/m2. Most of the participants (62.0%; n=186) had a BMI within the normal range, while 22.0% (n=66) were underweight and 12.7% (n=38) were overweight. Only 3.3% (n=10) were obese according to their calculated BMI values. The EAT-26 questionnaire analysis revealed that 6% (n=18) of the students had obtained a score of more than 20, suggesting abnormal eating behaviors (Table 2).12
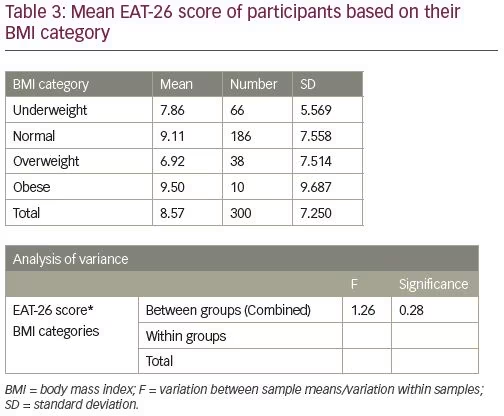
According to ANOVA test, there was insignificant difference between the groups in the mean score of EAT-26 (Table 3).
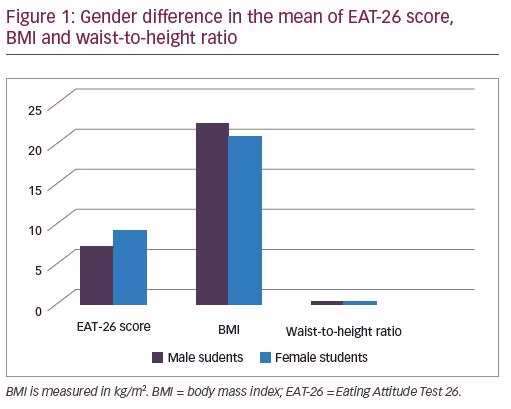
The independent t-test revealed that female respondents have a significantly lower waist–height ratio as compared with male respondents (p=0.01), and they scored significantly higher than males in the EAT-26 score (p=0.04). There was no gender difference in BMI of the study sample (Figure 1).
The eating behavior section of the EAT-26 scale indicated that out of the 300 students, 57.8% (n=173) felt that they were eating much more than most people would under the same circumstances and felt that their eating was out of their control. A total of 13.0% (n=39) and 13.3% (n=40) of the students induced vomiting or used laxatives, diet pills or diuretics, at least once within the previous 6 months to control their weight. It was also found that 65.3% of the students (n=196) exercised for more than 60 minutes per day to lose or to control their weight. Only 8.7% (n=26) had lost more than 10 kg in the past 6 months.
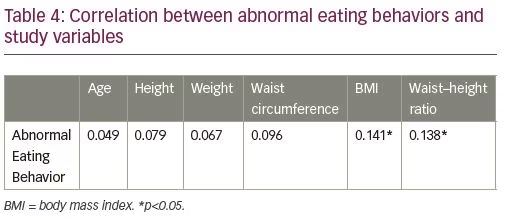
Spearman’s rank correlation coefficient was computed to find the relationship between abnormal eating behaviors and BMI, age, height, weight, waist circumference, and waist-to-height ratio. Table 4 denotes that there was no correlation between the abnormal eating behaviors with age, height, weight, and waist circumference. However, a positive correlation was found between abnormal eating behaviors and body mass index (rs=0.14, p=0.015), and between abnormal eating behaviors with waist-to-height ratio (rs =0.14, p<0.017), which indicates that an increase in BMI and waist-to-height ratio are associated with an increase in incidence of eating disorders.
To test whether the gender of the participants was associated with significantly different mean EAT-26 scores, an independent t-test was performed. There was a significant difference for gender t (298) = −2.59, p=0.01, with female students having higher scores (9.31 ± 7.79) than male students (7.23 ± 5.95).
Discussion
The present study reported a 6% prevalence of abnormal eating behaviors among students at MAHSA University. The majority of students (around 79.3% of the study sample) were from medical professional courses such as health and sports sciences, medicine and biomedical sciences, dentistry, pharmacy, nursing, and midwifery. The study findings showed a higher prevalence of abnormal eating behaviors among female students, which could be due to increasing societal pressure for females to maintain a low body weight. The body type many aspire to is to be thinner than ever before, yet the average weight of young women has increased, resulting in a discrepancy between the ideal body image and the actual body size of females, as shown in a study conducted among 657 female university students located in Seoul, Busan, Ulsan, Daejon, Chungcheongnam-do, and Gangwon-do, South Korea.11,12 This study reported lower BMIs in female Korean students than in female European and American Caucasian students; however, the dissatisfaction of female Korean students with their appearance was greater than that of the European and American students, indicating that more female Korean university students were suffering from an eating disorder.12 This is in agreement with another study conducted in an Indian medical school, which reported a 4.7% prevalence of eating disorders, all among females.13 In addition, a study conducted in the USA found a significantly higher prevalence of eating disorder symptoms, such as loss of control over eating, fasting, body avoidance, body checking, and binge eating, among women aged 18–35 years.14 A review of research concluded that although women seem to be at greater risk of developing eating disorders, the prevalence of such a problem is increasing among males, highlighting the importance of evaluating eating disorders among males as well.15,16
Our study showed a significant positive association between abnormal eating behaviors based on the EAT-26 score, BMI, and waist-to-height ratio. However, abnormal eating behaviors did not appear to be significantly related to age, weight, height, and waist circumference. This is contradictory to the findings of the cross-sectional study of disturbed eating attitudes and behaviors among 150 medical students conducted by Panchami et al. in Father Muller Medical College, Mangalore, Karnataka, India in 2016, which reported an absence of significant association between eating disorders and BMI.17 Our findings are also in contrast to those from a study conducted in India among adolescents in which no significant correlation between BMI and eating habits was reported.18 The difference may be due to the difference in age distribution, gender distribution, and demographic factors, and therefore needs further study. The proportion of participants in different categories of BMI was also different. In addition, the sample size that has been used in our study is double the size that was used in the Indian study, which could have contributed to the appearance of the correlation statistically. However, the association between BMI and EAT-26 reported in the current study were in accordance with the findings of a recent study conducted by Yousif et al. in 2019, whereby a significant association between BMI and eating behavior was reported among medical students.19 Disinhibition is an eating behaviour in which the subject tends to overeat in response to stress.19 The association between BMI and disinhibition was also reported in a more recent study conducted in the USA among 176 16-year-old adolescents, which reported that individuals with higher disinhibition had a higher BMI.20 The association between BMI and abnormal eating behaviors highlights the importance of psychiatric care for those with high BMI.21
In terms of predicting the consequences of being overweight or obese, measuring waist circumference and calculating waist-to-height ratio has been demonstrated to be of greater value than assessing BMI.22 The association between abnormal eating behaviors and waist-to-height ratio reported in our study is in agreement with the findings of a study conducted in Croatia among adults aged between 18 and 93 years, which reported that waist-to-height ratio is the most important anthropometric measure in terms of predicting lifestyle and psychological risks for obesity.23 Lifestyle factors such as the availability of convenience and fast food, study time patterns, and staying alone and away from home might contribute to abnormal eating attitudes. Lack of physical activity can also contribute to an increase in body weight and a resulting change in eating habits.24 A study conducted among the adult population in the UK has proved that waist-to-height ratio was able to identify more people at an early risk of the health consequences of obesity than other measures of obesity, such as waist circumference and BMI.25 Many studies have shown that obesity in adult age could be caused by various psychological risk factors during childhood, such as maltreatment, separation of parents or their death, and mental disorders, e.g., early onset major depressive syndrome, binge-eating disorders, and tobacco use.26–36
Limitations of the study and future research
The present study was conducted in one institution, MAHSA University. Future research conducted in a larger sample size that includes students from other institutions and fields of study are recommended to strengthen our conclusions and enable greater generalizability. Carrying out a longitudinal study, whereby the same study sample is observed repeatedly to obtain an accurate result, may also be of value to understand eating behaviors among students. The present study results showed an association between abnormal eating behaviors with BMI and waist-to-height ratio, but not causation; future research is encouraged to examine the causation of abnormal eating behaviors among students. Implementing nutrition and health awareness programs may benefit those who exhibit abnormal eating behaviors. Another limitation of the study is the use of the convenient sampling method; it is recommended to use random sampling in future studies.
Conclusions
In conclusion, among MAHSA students, female students are at greater risk of exhibiting abnormal eating behaviors than male students. The higher the BMI or waist-to-height ratio, the higher the prevalence of abnormal eating behaviors among the students in this Malaysian population.