




The World Health Organization (WHO) defines older adults as people aged 65 years or older.1 Today, older adults with diabetes mellitus (DM) are a growing population, with 33% of older adults meeting the criteria for DM.2 The risk of DM-related complications is elevated in this population; functional decline, comorbid conditions, hypoglycemia and polypharmacy-related adverse events cause significant burden to patients and their caregivers in managing DM.3,4 Clinicians face unique challenges in caring for older adults with DM, and professional societies have published guidelines to address these specific challenges.5 The use of technology, particularly DM technology, in older adults is an emerging research field, and there are growing data supporting their potential benefits in this population. The purpose of this review is to outline the role of technology in older adults, focusing on DM technology use, describing their barriers and potential benefits in these vulnerable patients.
A wide literature search was conducted on PubMed, with a focus on articles describing factors affecting the quality and safety of diabetes technology, as well as the effects of aging on older adults with DM. Furthermore, literature describing the use of insulin pumps and continuous glucose monitoring (CGM) in the older adult population was selected and reviewed. Finally, special attention was dedicated to the review of the literature relative to the barriers and benefits of technology in chronic disease management and specifically the literature relative to DM technology use in older adults. The results of our search are described in detail in the following sections.
Human factor systems, healthcare quality and patient safety in older adults with diabetes
The Systems Engineering Initiative for Patient Safety (SEIPS) model is a patient safety approach based on an industrial engineering subspecialty of human factors in healthcare. The more recent SEIPS 2.0. model incorporates three novel concepts: configuration, engagement and adaptation, where the patient is at the center of the work system; in this case, the elderly patient with DM, self-managing his or her chronic condition and related health needs, i.e., mitigating hypoglycemia.6 At the center of this model, the patient is part of a network in the work system and interacts with a multidisciplinary team (including family members, caregivers and healthcare professionals), in coordination with a healthcare organization to achieve a high quality of care and patient safety.
Medication adherence and safety are examples of work-process goals for an older adult with DM. Achieving these goals includes human factors such as patient knowledge, alertness and symptoms. The task includes DM self-monitoring, medication administration and insulin dose adjustment strategies based on blood glucose levels, nutrition, exercise and environmental factors. Many tools are available to achieve glycemic goals, while minimizing adverse outcomes (i.e., hypoglycemia). These tools range from glucose meters and pill boxes, to advanced technology such as CGM systems and insulin pumps.
Safe technology use requires family, caregiver, healthcare professional and interdisciplinary team coordination, where each ‘facilitator’ enables the patient to maintain DM self-care and safety at home. Together, these components create the external environment that allows the older adult with DM to achieve quality DM care at home with minimal risk of adverse outcomes. Of significance, for SEIPS model success, the patient requires intact cognition, knowledge, alertness, and the support of individuals and organizations.6,7 Conversely, if the patient has limited access to a supportive external environment or has decreased ability to self-manage DM due to decreased cognition, visual acuity, hearing loss or other impairments, these would constitute ‘barriers’ to the patient’s health and safety.6,7
Aging and the management of diabetes in older adults
Diabetes care is concentrated on the quest to achieve euglycemia and reduce short- and long-term complications. Glycated hemoglobin (HbA1c) reflects the average blood glucose over 2–3 months, is used to diagnose DM and has been the gold standard to measure treatment efficacy and predict the risk of long-term complications.8,9 However, in the older adult population with DM, several disorders, including red blood cell turnover, anemia and chronic kidney disease, affect HbA1c levels, often limiting its accuracy.5 Similarly, measurements of capillary glucose levels by fingerstick are also subject to inaccuracies and challenges due to equipment (glucose meter accuracy), physical (altitude and temperature) and patient factors (proper technique, hand washing, etc.). Therefore, accurate blood glucose monitoring may pose challenges in the older adult with DM, as it requires cognitive, visual and physical coordination.5
Several factors affect DM management in the older adult, starting with aging, which by itself affects the functionality of multiple organ systems, leading to significant impact on DM self-care, including cognitive, visual and hearing impairment, as well as impaired motor skills and dexterity.4 Cognitive impairment is present in up to half of all older adults with DM, and is associated with poor DM self-care, including diminished medication, diet and exercise adherence, as well as poor glycemic control and monitoring, with an increased risk of hypoglycemic episodes, which may in turn worsen cognitive impairment.10,11 Similarly, patients with DM have substantially higher prevalence of all-cause visual impairment when compared with those without DM,12 and the risk of diabetic retinopathy is increased in patients with type 1 DM (T1DM) and longer duration of DM.13,14 Furthermore, the increased prevalence of hearing impairment in people with DM is associated with poor functional status, depression, cognitive impairment and excess mortality.15 Conditions known to affect dexterity are common in older adults, and motor skills are negatively affected in older adults with DM.16 Older adults on complex DM regimens require advanced psychomotor function for routine blood glucose monitoring and medication administration; therefore, psychomotor function has a significant influence on performance of complex diagnostic and therapeutic plans in DM care.
Glycemic targets in the elderly
The Endocrine Society and American Diabetes Association’s (ADA) guidelines for older adults with DM recommend an assessment of overall patient health, including an evaluation of medical, functional, psychological, social and personal values, to guide individualized DM treatment goals and management strategies according to overall health status.3,5,17,18 In particular, these guidelines subdivide goals HbA1c for the healthy, intermediate and poor health groups as 7.0–7.5%, 7.5–8.0% and 8.0–8.5%, respectively,5 while at the same time recommending that the presence and quantification of episodes of hypoglycemia be ascertained at each visit.3 These considerations are especially important for older adults with T1DM, where self-administered insulin could become a significant challenge due to cognitive or functional impairment. In such cases, it is essential to include and educate family members and caregivers, as well as nursing home and long-term care facility staff in order to provide adequate and safe DM care.3
Hypoglycemia in the elderly
Hypoglycemia further complicates the treatment of DM in the older adult. Several factors place older adults at increased risk of hypoglycemia, including comorbidities, cognitive impairment, frailty, variable nutritional status, polypharmacy and hypoglycemia unawareness.4,19,20 Hypoglycemia rates increase with age and DM duration,4 and serious adverse events are associated with hypoglycemia in older adults.21 In addition, hospital admissions for hypoglycemia exceed those for hyperglycemia, with admission rates for hypoglycemia being two times higher in adults over 75 years.22 Older adults’ guidelines focus on mitigating hypoglycemia,3,5,18 and simplified or de-intensified regimens are recommended, in particular in patients with cognitive impairment.20,23 These have been shown to successfully reduce hypoglycemia without sacrificing glycemic control.23,24 In T1DM, it is especially important to avoid hypoglycemia due to increased risk of severe hypoglycemia and hypoglycemia unawareness in this population.25 In fact, the 2021 ADA Standards of Medical Care in Diabetes suggest that for older adults with T1DM, CGM may be another approach to reducing the risk of hypoglycemia,3 thus introducing the usefulness of DM technology in this population.
Barriers and benefits of technology in chronic disease management
mHealth
Advancements in technology offer innovative healthcare and health monitoring opportunities, including mobile health (mHealth), telemedicine and smart homes. mHealth technologies are emerging for chronic disease management and typically include smartphone-based interventions with integrated features, including applications, use of sensors, interactive touch screens and network connectivity.26 Smartphones and tablets offer a variety of mHealth applications, from self-management strategies (including self-monitoring, reminders and patient education tools) to health decision-making tools and social support strategies.26 mHealth applications and sensor devices have demonstrated a positive impact in prevention and clinical outcomes, including sensor devices offering accurate fall monitoring and detection,27–29 and smartphone communications leading to HbA1c reduction in patients with DM.30–32
While smart devices offer advancement in chronic disease monitoring, studies demonstrate adoption and usage of these technologies among older adults is inconsistent and low, and mHealth interfaces are infrequently tailored to meet the needs of the aging population.33–35
A framework (MOLD-US) has identified key factors influencing barriers to digital health adoption among older adults: cognition, motivation, physical ability and perception.36 Utilizing this framework, future technology development may identify mHealth usability concerns, and enhance designs tailored to the aging population, in an effort to minimize these barriers. Each component of this framework tackles common challenges to DM self-care in older adults by addressing errors in working memory (cognitive barriers), hand-eye coordination or dexterity (physical barriers), and auditory and visual acuity (perception barriers), all experienced by older adults with DM; as well as motivational errors, such as computer literacy.37
Telemedicine and the smart home
A potentially useful tool for older adults with DM includes telemedicine care, which may include an expanded team with integrated technology aimed to facilitate communication and improve patient outcomes. This area is rapidly expanding and may offer the enhanced support of DM technology in older adults in the future.38 Further technology includes the smart home, a personal residence equipped with inter-related software and hardware components able to monitor the environment and patient behaviors and activities via wearable medical sensors, actuators and communication technologies. It enables the monitoring of health and safety in the home, while maintaining patient quality of life, independence and comfort at a low cost.39 The smart home is designed for real-time monitoring, feedback and support of chronic medical conditions, including DM, and may serve as another component of increased use and support of DM technology in older adults.39
Diabetes technology
Diabetes technology is a broad term used to describe the hardware, devices, and software available for DM management, from blood glucose monitoring to insulin delivery devices.40 Tools used in DM technology primarily include CGM systems, continuous subcutaneous insulin infusion (CSII; or insulin pumps), and smart insulin pen devices and caps. CGM systems have evolved rapidly in the last two decades, with improvements in accuracy, longer sensor duration and ease of use; most are now approved for non-adjunctive use to make therapeutic insulin dose decisions without the need for confirmatory testing of glucose levels by fingerstick. With the recent advent of factory-calibrated sensors, CGM systems are likely to replace traditional self-monitoring of blood glucose (SMBG),41 thereby reducing the burden of frequent blood glucose measurements by fingerstick.42 CGM therapy is considered standard of care in patients with T1DM and insulin-treated type 2 DM (T2DM), and is endorsed by many professional societies.43,44 With alerts, alarms and glucose rate-of-change trend arrows, CGM systems predict glucose direction, which is especially beneficial in patients with a history of frequent hypoglycemia or hypoglycemia unawareness.40
Similarly, CSII systems have evolved into sophisticated tools that offer accurate insulin administration, even at very low doses. Insulin pump features include multiple programmable basal rate patterns, with on-demand basal rate modifications for physical activity or sick days. Insulin pump technology can reduce the burden of prandial insulin dose calculations through embedded bolus calculators, and allows programming of advanced boluses for complex meals.45
Several CGM and pump systems have become integrated either with sensor augmented pumps or with hybrid and advanced-hybrid closed loop systems.46 These systems have CGM-driven algorithms and can either suspend basal insulin delivery in response to a pre-set sensor glucose value, modulate the basal insulin delivery in response to predictive low sensor glucose value, fully automate basal insulin delivery and deliver correction boluses in response to sensor glucose-driven thresholds.47,48 Multiple professional societies have endorsed the use of CGM and CSII in patients with T1DM and T2DM as tools to reach lower HbA1c in patients not meeting glycemic targets, decrease hypoglycemia and glycemic variability, as well as to improve time in target range.3,40,43,44,49
The clinical benefits of CGM and CSII therapy in children and adults are well established, and include reduction of daytime and nocturnal hypoglycemia and improvement of HbA1c without increase in hypoglycemia, regardless of the method of insulin delivery.50–56 Of note, the use of CGM therapy has also shown to improve DM-specific quality of life measures,57 and significantly reduce the glycemic fluctuations and glycemic variability in T1DM and T2DM, increasing the percentage of time spent in target range (70–180 mg/dL or 3.9–10 mmol/L).40,43,50
Recently, connected pens or ‘smart’ pens, have become available; these are reusable pens and require the insertion of insulin cartridges. Several models are available, some of which are equipped with near-field communication technology, bolus memory or the ability to record the last insulin dose, and can be used for both basal and mealtime insulin.58 Other smart pens are used for mealtime insulin only, and can record the amount and timing of each insulin dose. They transmit the information via Bluetooth to a smartphone application with a bolus calculator, which also includes insulin on-board information, and users can manually enter additional information into the application, such as long-acting insulin dose.59–61 Both brands can be downloaded into various data visualization programs for healthcare professionals. Some insulin pens can be fitted with various brands of insulin caps, able to record insulin dose, time elapsed or missed doses.59 The use of connected insulin pens together with CGM has shown benefits, including increased time spent in target range, reduced time in level 2 hypoglycemia and reduced frequency of missed boluses.58
Benefits and barriers of diabetes technology use in older adults
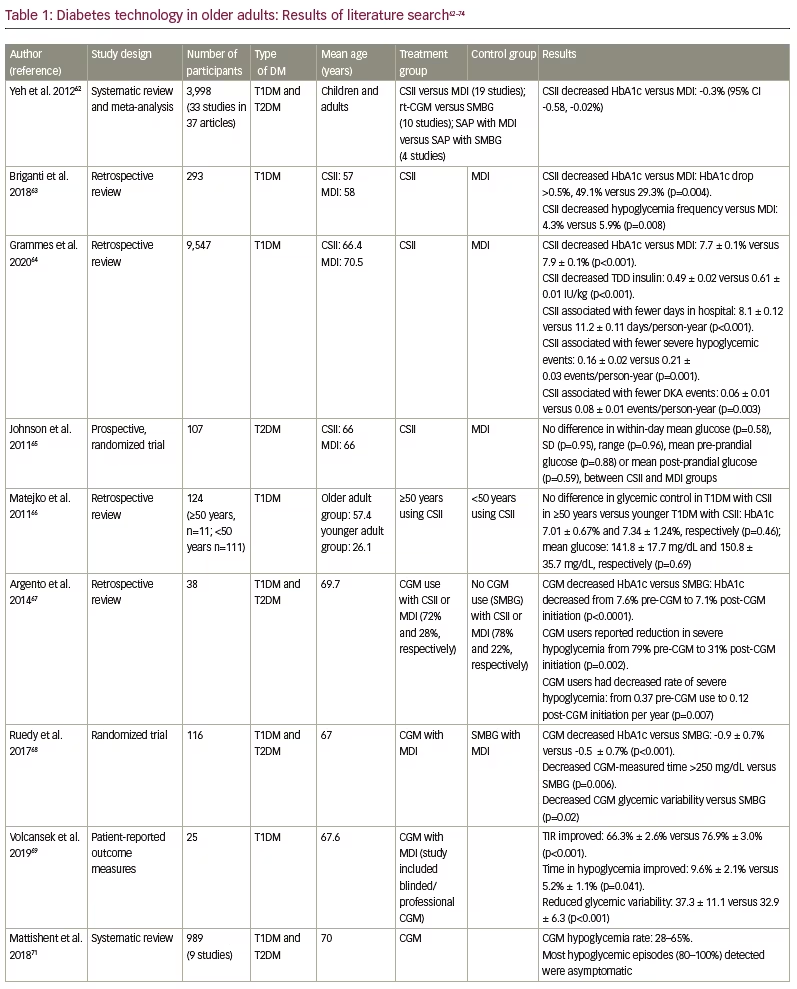
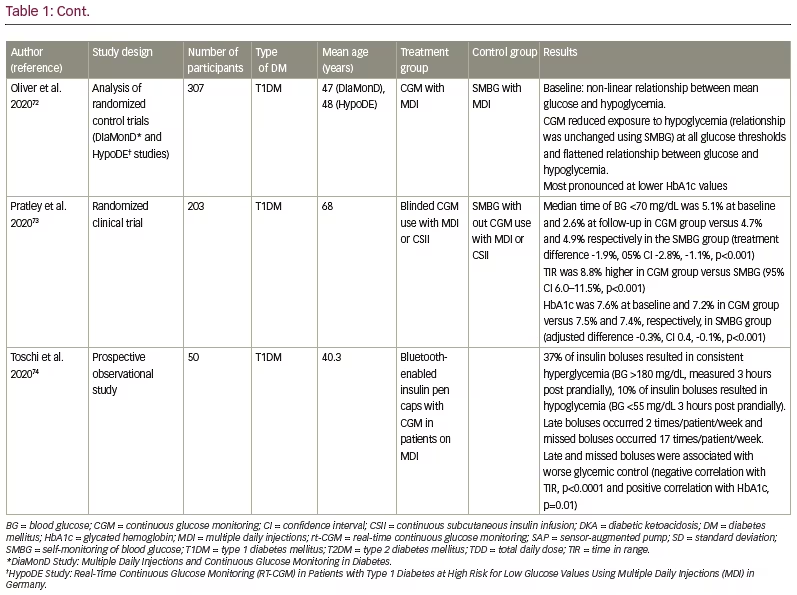
Historically, the literature on the use of DM technology in older adults has been limited. Recently, however, data are emerging on the benefits and challenges of its use in this age group. Table 1 outlines the studies that have enrolled older adults using either insulin pumps or CGM, or both, and their results.
Benefits
Continuous subcutaneous insulin infusion
Generally, insulin pump studies and meta-analyses have determined that CSII has modest advantages over multiple daily injections (MDI) for HbA1c lowering in T1DM (-0.30% [95% confidence interval {CI} -0.58, -0.02]) and reduction in severe hypoglycemia rates.40,62 When focusing on data in adults with T1DM ≥50 years old, CSII has been associated with improved glycemic outcomes (HbA1c reduction) and a trend toward less hypoglycemia when compared with age-matched adults on MDI.63 A retrospective analysis of patients with T1DM ≥60 years old showed lower HbA1c and daily insulin dose, as well as decreased hypoglycemia, number of days in the hospital and diabetic ketoacidosis compared with those using MDI.64 A cohort of adults with T2DM aged >60 years, comparing CSII to MDI, found no difference in glycemic variability measured by CGM.65 Similar results were found when comparing young adults with T1DM to older adults with T1DM using CSII.66
Continuous glucose monitoring
While the literature on insulin pump therapy in older adults remains limited, evidence from CGM use in older adults has expanded in the last 5 years, and its benefits have been analyzed in a variety of settings. In older adults with T1 and T2DM, the use of personal CGM was associated with a decrease in mean HbA1c and reduced severe hypoglycemia compared with pre-personal CGM use.67 In a randomized clinical trial comparing CGM versus SMBG in older adults (≥60 years) with T1 or T2DM using MDI, results showed a reduction in HbA1c and glycemic variability, as well as increased time spent in target range in CGM users. There was minimal hypoglycemia observed in the CGM group, and high CGM satisfaction from patient questionnaires.68 Acceptability of CGM in elderly patients with T1DM and T2DM has also been studied; increase of time in range, decrease time in hypoglycemia and hyperglycemia, and a reduction of glycemic variability were observed. In addition, high levels of satisfaction, and improved sense of security were reported for CGM users.69
Studies clearly demonstrate the increased incidence of hypoglycemia and poor outcomes associated with hypoglycemia in older adults; however, it has also been shown that relaxed HbA1c targets do not protect against hypoglycemia in this population.70 CGM offers increased recognition of hypoglycemia, as evidenced by a systematic review of CGM use in 989 older adults (aged >65 years), demonstrating high rates of hypoglycemia (28–65%), the majority of which were asymptomatic (80–100%).71 Furthermore, analyses of patients with T1DM on MDI demonstrate that real-time CGM results in an attenuated relationship between time spent in hypoglycemia and overall glucose control compared with SMBG, whereby the relationship is unchanged. This was most pronounced at lower HbA1c values, highlighting the ability to achieve target glucose using CGM without significant hypoglycemia exposure.72 In the Wireless Innovations for Seniors with Diabetes Mellitus (WISDM) clinical trial, CGM use was compared with SMBG in adults >60 years with T1DM, to determine the effects on hypoglycemia reduction in CGM users. Decreased time spent in hypoglycemia was seen in CGM users versus SMBG, as well as improved time in target range and HbA1c in the CGM group versus SMBG group.73 These studies highlight the prevalence of hypoglycemia in older adults and underscore the frequent hypoglycemia unawareness in patients with longstanding DM, and demonstrate the need for efforts to mitigate time spent in hypoglycemia range, which can be offered by CGM.73
Smart pens
Digital health technologies are rapidly expanding, and emerging studies of smart pens demonstrate the utility of information these technologies provide, including a greater understanding of insulin dose timing and glucose control. In a recent study of Bluetooth-enabled insulin pens and concomitant CGM use in patients on MDI, late boluses occurred 2 times/patient/week and missed boluses occurred 17 times/patient/week. Late and missed boluses were associated with worse glycemic control.74
Barriers
Barriers to adoption of DM technology use in older adults include challenges such as ‘human factors’, including the attitudes, perception and preferences of the patient, family/care giver and/or DM care team regarding DM technology use. Adults with DM, including older adults, have shown concerns about the hassles of wearing a device, and a dislike of devices on their body.75 In a study evaluating perceptions of DM technology in middle-aged to older adults with T2DM (53–72 years), CGM use was associated with increased physician guidance and participant motivation;76 this study highlights the role of identifying modifiable factors that may engage and support use of DM technology in older adults.
Continuous subcutaneous insulin infusion
Despite the reported benefits of CSII therapy in older adults, these individuals face additional challenges relative to the requirements for CSII and related supplies coverage by the US Centers for Medicare and Medicaid Services (CMS). In a survey of 241 older adults with T1DM on Medicare, 57.7% reported issues with obtaining supplies due to a delay in the release of supplies, difficulty getting the necessary paperwork completed and challenges seeing a healthcare provider every 90 days. Due to these challenges, participants reported changing behaviors, including leaving site in place for more than 3 days (64%) and reusing pump supplies (34%). As a result, participants reported adverse outcomes including more erratic glucose levels (48%) and pain/irritation at infusion sites (34%).77 Additionally, in small published case reports, although patients with T1DM and dementia benefitted from the use of insulin pump therapy or CGM in an assisted living facility, there was considerable time spent in intensive training for the staff, the patient and family, to safely and successfully use this technology.78
Continuous glucose monitoring
Similar to CSII coverage challenges, CGM access has been historically problematic for older adults. Prior to January 2017, access to CGM for US Medicare beneficiaries with DM was severely limited by lack of coverage. A survey evaluated health and quality of life associated with CGM use in adults ≥65 years with T1DM or T2DM on insulin therapy, and compared findings with adults unable to obtain CGM due to insurance limitations (‘hopefuls’). CGM users reported fewer moderate and severe hypoglycemic episodes (p<0.01), as well as improvements in quality-of-life scores (p<0.001), including improved wellbeing, less fear of hypoglycemia and less DM distress, compared with hopefuls.79 Similar results on improved rates of hypoglycemia and quality-of-life scores in patients with T1DM using CGM compared with hopefuls have been reported, providing additional evidence to support CGM use in older adults.80 Since January 2017, CGM coverage is available to CMS beneficiaries with DM, treated with at least three insulin injections per day, measuring glucose levels by fingerstick four times per day and requiring frequent insulin adjustments, which has expanded access to CGM in this population.81
Overcoming diabetes technology barriers in older adults
While several factors represent barriers to adoption of DM technology, it is noteworthy that among patients with T1DM, there is increased treatment satisfaction transitioning from traditional to advanced technology use (CSII and CGM),68,69,82 with increased feelings of safety (by preventing hypoglycemia), as well as improved wellbeing with CGM use in older adults with T1DM.81 Of note, the results of these studies emphasize how there are different populations of older adults with DM, and whereas some people with DM have cognitive decline and multiple comorbidities, many individuals with long-standing DM are still living independently, have few comorbidities and are able to learn these new technologies and manage them successfully.69,70
In addition, psychosocial DM technology research has begun to outline interventions focused on minimizing barriers to DM technology use, and augmenting education programs aimed to facilitate technology adoption for those individuals who may have age-related challenges.83 Further research based on the MOLD-US usability framework for mHealth technology development will be critical in considering programs tailored to the needs of older adults’ diminishing cognition skills, physical ability and motivational barriers to technology use.36,37 Taken together, all these reports strongly suggest that the use of DM technology is beneficial in older adults with DM. How, then, do we reconcile the multiple potential barriers these patients face due to their age-related complications; cognitive, visual and hearing impairment; and/or impaired dexterity?
These barriers should not preclude the use of DM technology in older adults with sub-optimal glycemic control when the potential for improved outcomes may be achieved with DM technology. In the setting of the challenges outlined above, the importance of individualized education and training on DM technology systems (whether CGM, insulin pump or DM applications) cannot be over emphasized. As elegantly discussed by Toschi and Munshi, DM technology in the older adult should aid in improving quality of life and lower the risk of hypoglycemia.84 Therefore, in these situations, it is crucial for the clinician, the patient and the caregiver (if necessary), to identify the appropriate technologies and complete education sessions to ensure that the patient and caregiver are comfortable with these tools, and are able to troubleshoot situations, such as malfunction, using protocols to obtain assistance (whether by customer services or the diabetes care and education specialist) within clinical practices. In addition, offering simplified instructions with periodic reassessment of the capacity for safe and appropriate use in these patients contributes to the success and user satisfaction, while at the same time uncovers specific challenges that may have not been recognized in the initial training.84
Therefore, the use of chronic care and DM technology in older adults should be a multidisciplinary effort, especially if the patient is living in long-term care facilities, ensuring the ability to manage and troubleshoot DM technology when initiating this type of therapy.40,85 Furthermore, advances in chronic disease management, including telemedicine and the smart home, offer exciting opportunities for older adults to receive increased monitoring and communication, and enhanced support of DM technology and DM management.
Conclusion
The incidence and prevalence of DM is increasing and is expected to continue on an upward trajectory as the adult population with DM ages. Older adults with DM are at high risk of DM-related complications, geriatric syndromes, functional impairment and increased mortality with longer duration of DM. Common comorbid conditions in older adults with DM include cognitive, visual and hearing impairment, as well as hypoglycemia and polypharmacy; these conditions add complexity and special considerations to DM care plans. Guidelines recommend careful evaluation of individual medical, functional, psychological, social and personal values, to guide DM treatment goals and management strategies. Evidence is building in the literature regarding the benefits of the use of DM technology in older adults. Patient satisfaction is usually high in people with DM who live independently and are able to successfully self-manage their condition. At the same time, an individualized approach to the education and training of the frail, older DM population needs to be implemented, and patients may require the support of their families to successfully use DM technology. Finally, technology, and DM technology in particular, is advancing at a fast pace and offers promises for care enhancement in older adults with DM. It also has the potential to be a very valuable tool in vulnerable older adults if used appropriately to reduce hypoglycemia and enhance safety.


