Statin-associated muscle symptoms (SAMS) may lead to medication non-adherence among statin users. SAMS include myalgia, myositis and rhabdomyolysis (rarely seen).1 According to a recent study conducted in India, about 22% of statin users are affected by SAMS.2 Many studies have been conducted to establish a correlation between SAMS and levels of vitamin D and creatine phosphokinase (CPK; a marker of muscle damage), but the exact mechanism is not yet clear.3–5 It has been documented that statins can affect vitamin D levels; low-density lipoprotein cholesterol (LDL-C) is a vitamin D carrier and statins, by reducing LDL-C, could decrease vitamin D levels.6 However, to complicate this, some statins and vitamin D are metabolized by the CYP3A4 enzyme; hence by competing for binding with CYP3A4, statins could increase levels of vitamin D.6,7
While there is evidence that vitamin D supplementation can reduce myalgia,8 most clinical studies have produced mixed results regarding the relationship between SAMS and vitamin D levels.5,6,9,10 Hence there is a complex relationship between SAMS, vitamin D and LDL-C levels. Moreover, studies evaluating the relationship between LDL-C levels, vitamin D levels and SAMS are currently limited. The main objective of this study was to establish the relationship between SAMS and levels of vitamin D and LDL-C.
Methods
Study design, study setting and ethics
This single-centre, cross-sectional, comparative, observational study was carried out from 26 June 2018 to 28 September 2018, in the Departments of Cardiology, Pharmacology and Biochemistry of the Government Medical College and Hospital, Chandigarh, India, after obtaining permission from the Institutional Ethics Committee (vide letter No. IEC/2018/97). The study was carried out according to the principles of Good Clinical Practice and the Declaration of Helsinki. Male and female patients visiting the cardiology outpatient department who had been prescribed statins, irrespective of the indication, were included in the study. However, those with onset of myalgia before commencement of statin treatment, traumatic injuries, fever, viral or bacterial infections, arthritis of any type and other conditions presenting with muscular pain, and those who were not willing to give written informed consent, were excluded.
Eligible patients attending the cardiology outpatient department of our institute, fulfilling the inclusion criteria and having none of the exclusion criteria, were approached. The objective and the methodology were explained to the participants and, if they agreed to participate, written informed consent was obtained. A thorough medical history was taken (details pertinent to personal information, disease and medicines and other treatment modalities, concomitant diseases and medications, duration of statin use) and a clinical examination was conducted, after which, individual SAMS were recorded in case-report form. In order to conduct laboratory investigations, 5 mL of blood was withdrawn from each patient in aseptic conditions.
Biochemical estimations
Relevant laboratory investigations, including vitamin D levels, CPK levels, and LDL-C levels, were performed for all patients. Vitamin D was estimated by a fully automated chemiluminescence system (ADVIA Centaur XP, Siemens, Munich, Germany) using the specific kit. This estimation is based on competitive immunoassays as described by Thienpont et al.11 Vitamin D levels were classed as deficient (<20 ng/mL), insufficient (20–30 ng/mL) and sufficient (>30 ng/mL). CPK estimation was done using a Roche Modular P800 chemistry analyser (Roche, Basel, Switzerland) using the specific kit. The coefficient of variation (within run) for vitamin D estimation test was ≤8%. The method, recommended by the International Federation of Clinical Chemistry, comprises the quantitative estimation of CPK using enzyme assays. The method and its principle are described in detail by Hørder et al.12 The reference range for CPK is 20–200 IU/L in males and 20–180 IU/L in females.13 LDL-C estimation was done using an enzymatic colorimetric assay on the Roche Modular P800 chemistry analyser. The principle and the method have been described in detail by Pisani et al.14
Statistical analysis
Based on two previous estimates considering a two sample proportion test for equality with an alpha error of 5%, power of 80%, the difference of proportions of 0.21 and prevalence of SAMS as 22%, the desired sample size was calculated to be 246: with 54 statin users with SAMS and 192 patients without SAMS.2,15 Data were analysed using statistical software, ‘SYSTAT’ Statistics for Windows version 13. Categorical data were analysed using Chi square test and Fisher’s exact test. Continuous variables were analysed by using t-test (for parametric data) or
Mann–Whitney U test (for non-parametric data). Data were represented as numbers, percentages, mean ± standard deviation (SD) and median (range).
As most of the Indian population have insufficient levels of vitamin D,16 in order to reflect a more accurate prediction of the relationship between SAMS and vitamin D levels, the levels of vitamin D were converted into percentiles and univariate analysis was performed for different percentile cut-off values with respect to SAMS and represented in terms of odds ratio (OR) with 95% confidence interval (CI). Similar percentile cut-offs were also generated for LDL-C. Receiver operating characteristic (ROC) curve analysis was used to predict the relationship between vitamin D, LDL-C and SAMS. We also performed multivariate analysis using binary logistic regression. P<0.05 was considered statistically significant.
This original reseach article was prepared according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies.17
Results
Demographic characteristics of the participants
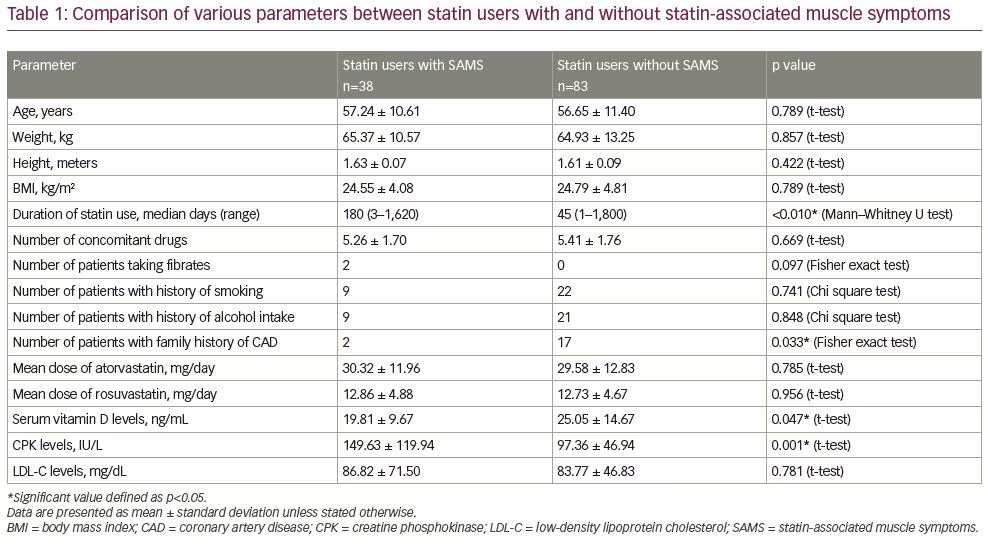
The predicted sample size required for this study was 246; however, due to the institutional and funding constraints and the limited period for study completion, we were able to enrol 121 patients (38 with SAMS and 83 without SAMS). Of all the patients, 72 were male and 49 were female. The mean age of participants was 56.83 ± 11.12 years, mean weight was 65.0 ± 12.4 kg, mean height was 1.62 ± 0.09 m, and mean body mass index (BMI) was 24.72 ± 4.57 kg/m2. Mean age, weight, height, BMI and other characteristics of statin users with and without SAMS are presented in Table 1.
Prescribing pattern of statins
Atorvastatin and rosuvastatin were prescribed to 103 (85.1%) and 18 (14.9%) patients, respectively. Mean doses of atorvastatin and rosuvastatin prescribed were 29.81 ± 12.52 mg and 12.78 ± 4.60 mg, respectively. Mean doses of atorvastatin and rosuvastatin prescribed among statin users with and without SAMS are given in Table 1. Median duration of statin use was 60 days (range 1–1,800 days). Median durations of statin use among patients with and without SAMS are given in Table 1.
Statin-associated muscle symptoms
Thirty-eight (31.4%) participants were found to have SAMS: out of these, 23 were male and 15 were female patients. The difference in occurrence of SAMS among male and female statin users was not found to be statistically significant (p=0.877). Thirty-one (30.1%) atorvastatin users and seven (38.9%) rosuvastatin users were found to have SAMS (p=0.458). Twenty-eight participants presented with myalgia, four with myositis (myalgia with elevated CPK) and six with asymptomatic elevation in CPK levels (without myalgia).
Onset and location of myalgia
Of the 32 patients who developed muscular pain (28 with myalgia and 4 with myositis), the mean time of onset of muscular pain after statin use was 6.62 months, and the median time of onset of muscular pain was 1.4 months (range 0.13–23.77 months [4–713 days]). Twenty-four participants had muscular pain affecting predominantly the lower limbs, three predominantly of the upper limbs, and five reported muscular pain over both upper and lower limbs.
Vitamin D and its relationship with statin-associated muscle symptoms
Mean vitamin D levels of all participants were 23.40 ± 13.49 ng/mL.
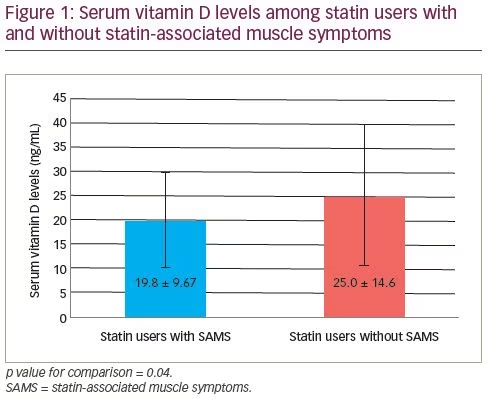
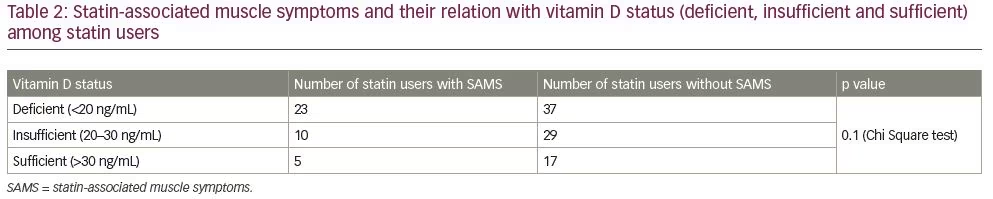
Significantly lower serum vitamin D levels were found among those presenting with SAMS compared with those without SAMS (19.81 ± 9.67 ng/mL versus 25.05 ± 14.67 ng/mL, mean difference of -5.25, 95% CI -10.41 to -0.07, p=0.047) as shown in Figure 1. Sixty patients had vitamin D levels <20 ng/mL (i.e., deficient), 39 had vitamin D levels 20–30 ng/mL (i.e., insufficient) and 22 had levels of >30 ng/mL (i.e., sufficient). The distribution of the three categories of vitamin D levels and their relation with SAMS was not found to be statistically significant, as shown in Table 2.
Creatine phosphokinase levels
Mean CPK levels of all participants were 113.78 ± 80.83 IU/L. Ten statin users were found to have elevated CPK levels (with mean levels of 302.80 ± 138.23 IU/L). Significantly higher levels of CPK were observed among patients with SAMS compared with those without SAMS (149.63 ± 119.94 IU/L versus 97.36 ± 46.94 IU/L, mean difference of 52.27 IU/L, 95% CI 22.25–82.29 IU/L, p<0.01).
Low-density lipoprotein cholesterol and its relationship with statin-associated muscle symptoms
Mean LDL-C levels of all participants were 84.7 ± 55.2 mg/dL. Ninety-nine participants had LDL-C levels <100 mg/dL, which is considered the target level for patients with coronary artery disease. No significant difference was observed in LDL-C levels among statin users with and without SAMS (86.82 ± 71.50 mg/dL versus 83.77 ± 46.83 mg/dL, p=0.781). Thirty-two patients out of 99 with LDL-C levels <100 mg/dL, and six patients out of 22 with LDL-C levels ≥100 mg/dL, were found to have SAMS (p=0.644).
Relationship between statin-associated muscle symptoms, vitamin D levels and LDL-C levels
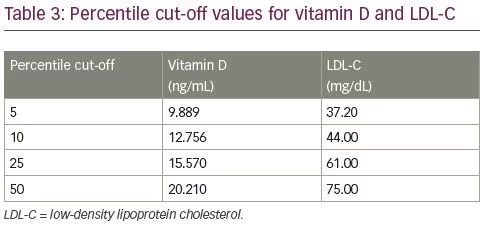
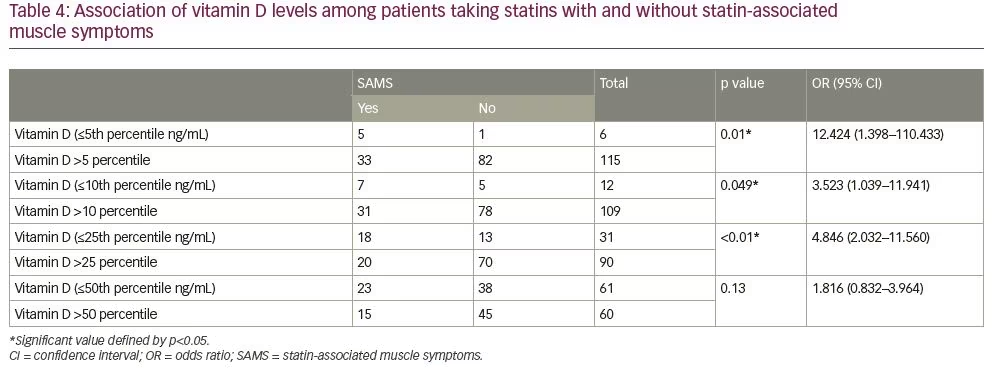
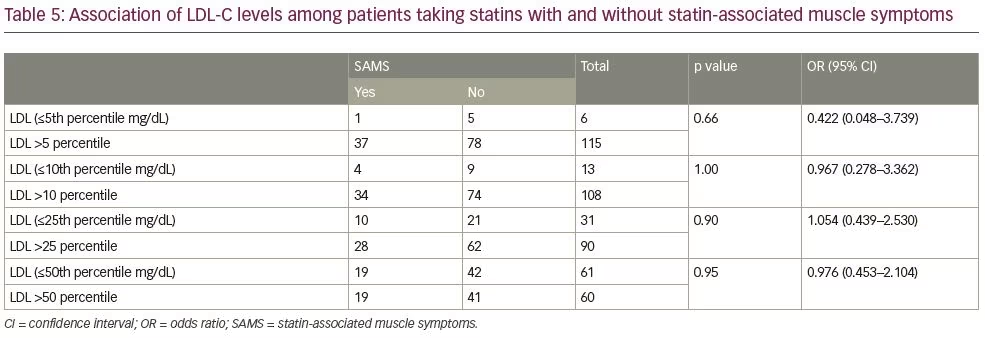
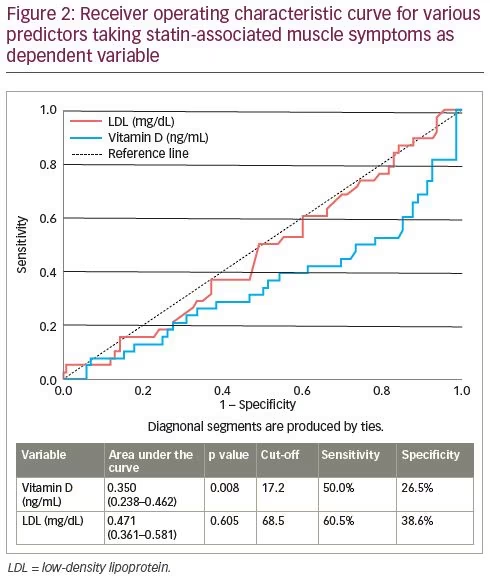
Cut-off percentile values for vitamin D and LDL-C are shown in Table 3. Taking different percentile cut-off levels for vitamin D and LDL-C (5, 10, 25 and 50), an association with SAMS was seen in terms of OR. With vitamin D levels less than or equal to the 5th, 10th and 25th percentiles, the chances of occurrence of SAMS were significantly raised by 12.42, 3.52 and 4.80 times compared with those with vitamin D levels more than the 5th, 10th and 25th percentile cut-offs, respectively (Table 4). Various percentile cut-off values of vitamin D and their relationship with SAMS are shown in Table 4. However, similar cut-off percentiles for LDL-C did not show any conclusive relationship with SAMS (Table 5). ROC curves were drawn with vitamin D and LDL-C as predictors and SAMS as a dependent variable. With vitamin D levels of ≥17.2 ng/mL, the sensitivity and specificity of predicting SAMS were 50% and 26.5% (area under curve [AUC] 0.350, p=0.008; Figure 2), respectively. With respect to LDL-C, AUC was 0.471 (p=0.605).
We did not find any significant relationship between the risk of occurrence of SAMS (dependent variable), vitamin D (OR 0.95, 95% CI 0.91–1.01, p=0.083), LDL-C (OR 1.0, 95% CI 0.99–1.01, p=0.959), age (OR 1.0, 95% CI 0.97–1.04, p=0.754), gender (female OR 1.63, 95% CI 0.64–4.15, p=0.308) or BMI (OR 0.97, 95% CI 0.88–1.06, p=0.543). However, there was a significant association between risk of SAMS and CPK levels. Each unit increase in CPK levels led to a 1% increase in the risk of developing SAMS (OR 1.01, 95% CI 1.003–1.019, p=0.007).
Discussion
This study was undertaken to establish a relationship between SAMS and levels of vitamin D and LDL-C. The prevalence of SAMS among the statin users enrolled in this study was 31.4%. In a recent study conducted in India, Singh et al.2 reported the occurrence of SAMS in 22% of geriatric statin users. In another Indian study, Mulchandani et al.18 reported myalgia in 32% of statin users. In the present study, significantly higher levels of CPK (a marker of muscle injury) were observed among patients with SAMS compared with those without SAMS. This further strengthens the association of statin use and likelihood of occurrence of SAMS.
The observed mean onset of myalgia pain after statin use in our study (6.6 months) was similar to that of a study by Hansen et al., which reported 6.3 months; however, we observed an earlier, shorter range of onset: 4 days to 2 years, compared with 1 week to 4 years.19
Significantly lower levels of vitamin D were observed among patients who presented with SAMS compared with those who did not (Figure 1); a finding that is consistent with previous studies.4,5,8,9 However, when we separated patients into groups based on their vitamin D status as deficient (<20 ng/mL), insufficient (20–30 ng/mL) or sufficient (>30 ng/mL), there was no significant difference between the number of patients in each group with respect to the occurrence of SAMS. Taylor et al. also found that vitamin D deficiency or insufficiency and changes in vitamin D levels during statin therapy did not predict the occurrence of SAMS.20
As the current study was conducted in India, and many Indian people have insufficient levels of vitamin D, we converted their levels into percentiles, which revealed that the chance of occurrence of SAMS was significantly increased in those with vitamin D levels less than or equal to the 5th, 10th and 25th percentiles. This association was not significant at a percentile cut-off level of 50, which corresponds to vitamin D levels of ≥20.12 ng/mL. This gives a meaningful conclusion that as vitamin D levels increase, there is less likelihood of the occurrence of SAMS.
Hence, vitamin D deficiency may exacerbate SAMS in statin users. A study by Riche et al. also found that deficient levels of vitamin D are significantly associated with SAMS, and that patients with vitamin D levels >20 ng/mL had a lower risk of SAMS compared with those with vitamin D levels of ≤20 ng/mL.3 In a study by Bittner et al., 49% of atorvastatin users at baseline and 56% at 1 year, had vitamin D deficiency, and myalgia was present in 8.3% of vitamin D-deficient subjects.21 Similar results were recently reported by the Pennisi et al., who observed a significant relationship between vitamin D deficiency and SAMS.22
In the present study, no association was found between the occurrence of SAMS and LDL-C levels. This is in agreement with the findings of a study by Piantanida et al. who reported no significant difference in LDL-C levels among patients with vitamin D levels <10 ng/mL, 10–20 ng/mL and ≥20 ng/mL.23 The average LDL-C levels in our study were found to be <100 mg/dL in both groups, i.e., statin users with SAMS and statin users without SAMS. Additionally, no association was found between the levels of LDL-C (<100 mg/dL and ≥100 mg/dL) and the occurrence of SAMS among statin users. There is paucity of data on the occurrence of SAMS and its prediction by the levels of LDL-C. There are certain theoretical concerns of a likelihood of association between LDL-C and occurrence of SAMS, as LDL-C is a vitamin D carrier and statins, by reducing LDL-C, could decrease vitamin D levels;6 however, statins and vitamin D are metabolized by the CYP3A4 enzyme. By competing for CYP3A4, statins may increase levels of vitamin D.6,7 Schwartz observed that during vitamin D supplementation (800 IU/day for 6 weeks), the concentration of atorvastatin, active metabolites, LDL-C and total-cholesterol remained lower, yet she also concluded that vitamin D showed a synergistic effect to atorvastatin in reducing lipid parameters.24 Pérez-Castrillón et al. reported that in patients with insufficient and normal vitamin D levels, a good response to atorvastatin therapy was shown, compared with those who had deficient vitamin D levels.7 They concluded that sufficient vitamin D concentrations may be essential for atorvastatin to control lipid levels in patients with acute myocardial infarction. However, no such findings were observed in our study, as in both groups (statin users with SAMS and statin users without SAMS), LDL-C levels were in control. Hence, we are not able to comment on the likelihood of such an interaction. With vitamin D as a variable, the sensitivity and specificity (at a cut-off level of 17.2 ng/mL) of predicting the occurrence of SAMS were 50.0% and 26.5%, respectively (Figure 2). This discrimination, although significant (p=0.008), lacks any strong association. LDL-C had a moderate discrimination (AUC=0.471); however, this was not significant (Figure 2).
The data regarding the association of levels of vitamin D and LDL-C with SAMS are somewhat mixed. Our study attempted to explore this relationship; however, our conclusion must be regarded with caution due to the small sample size and cross-sectional nature of our study. As most of the population in the Indian subcontinent are deficient in vitamin D, assessment of vitamin D as a major predictor of SAMS requires subdivision into smaller values (percentiles) to provide a clear picture among those who have a higher degree of vitamin D deficiency.16,25 We highlighted the occurrence of SAMS among patients with the lowest levels of vitamin D in an Indian population that is already
vitamin D deficient.
The limitations of this study include a small sample size, which was due to the time constraints, as the project was to be completed within a restricted period of 3 months, and reduced availability of vitamin D kits due to funding constraints. Another limitation includes the cross-sectional nature of the study, as a prospective study in the assigned duration for completion and submission of the project was not feasible. The chemiluminescence method of vitamin D estimation, used in this study, has a drawback of over-reporting vitamin D deficiency due to poor traceability to the reference method (mass spectrometry).26 Another limitation of the study is the measurement of vitamin D in patients with dyslipidaemia. As vitamin D is a lipophilic substance and is particularly vulnerable to the presence of other lipids, especially triglycerides, in the serum or plasma sample, this can change the ability of the binding agent to associate with vitamin D in the sample; this can produce variability in the measurement.
Conclusion
We can conclude that statin users with low levels of vitamin D are at increased risk of developing SAMS; this risk decreases with higher levels of vitamin D. However, due to the observational nature of this study and other limitations, further randomised interventional studies are needed to verify these findings. LDL-C status of statin users failed to predict any meaningful association with SAMS. Further large-scale prospective studies are required to investigate the exact relationship between these parameters.