In 1980, the brothers Cedric and Frank Garland proposed the ultraviolet-B (UVB)–vitamin D–cancer hypothesis after observing that US colon cancer mortality rates were lowest in the sunny southwest and highest in the least sunny northeast.1 The evidence that UVB irradiance and vitamin D reduce the risk for many cancers continues to increase. As of March 16, 2013, PubMed included 3,036 entries with vitamin D and cancer in the abstract or title.
In 1980, the brothers Cedric and Frank Garland proposed the ultraviolet-B (UVB)–vitamin D–cancer hypothesis after observing that US colon cancer mortality rates were lowest in the sunny southwest and highest in the least sunny northeast.1 The evidence that UVB irradiance and vitamin D reduce the risk for many cancers continues to increase. As of March 16, 2013, PubMed included 3,036 entries with vitamin D and cancer in the abstract or title. Evidence supporting this hypothesis comes from a variety of studies: ecological, observational, record-linkage, cross-sectional, laboratory, and randomized controlled trials (RCTs). This paper briefly reviews the evidence.
Solar Ultraviolet-B
Ecological studies of cancer incidence and mortality rates using indices of solar UVB doses provide the strongest evidence to date that vitamin D reduces the risk for many cancers. A US study using solar UVB doses at the earth’s surface for July 1992 (determined with a NASA satellite instrument) inversely correlated the mortality rates of 15 cancers with this UVB index.2 That paper included graphs showing that cancer mortality rates for bladder, female breast, and all cancer, less gastric cancer, had nearly linear inverse relations with solar UVB doses for 500 state economic areas, with a slight hint of leveling off at the highest doses. A later study that added other riskmodifying factors (i.e., alcohol consumption, Hispanic heritage, poverty level, smoking, and urban/rural residence) confirmed the results of the first study regarding UVB doses.3 The findings for alcohol consumption and smoking in that study agreed well with what was known then about both’s role in cancer risk. A prospective study of cancer incidence rates for residents of seven states in the US found that living in a state with higher solar UVB doses was associated with increased risk of melanoma and reduced risk for bladder, colon, kidney, squamous-cell lung, pleural, and prostate cancer, as well as non-Hodgkin’s lymphoma, with indications of reduced risk for pancreatic and thyroid cancer.4
Recently a study reported the effects of alcohol consumption on cancer mortality rates, identifying the cancers most affected and that alcohol accounted for about 3.5 % of all cancer deaths.5 The findings in the multifactorial ecological study agreed well with this study.
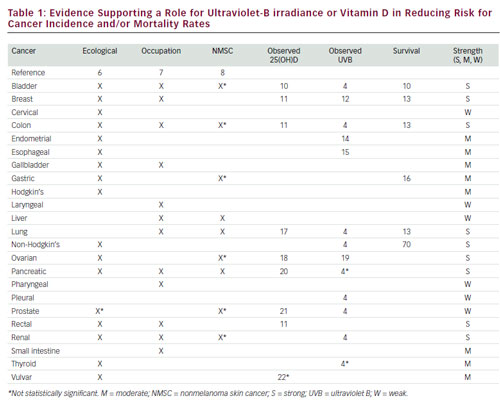
Many single-country ecological studies have generally made similar findings by using solar UVB doses or latitude as the index of serum 25-hydroxyvitamin D [25(OH)D] concentration. I recently reviewed such studies from Australia, China, France, Japan, and Spain.6 Cancers with the strongest evidence include bladder, breast, cervical, colon, endometrial, esophageal, gastric, lung, ovarian, pancreatic, rectal, renal, and vulvar cancer, as well as Hodgkin’s and non-Hodgkin’s lymphoma. Weaker evidence exists for nine other cancers: brain, gallbladder, laryngeal, oral/ pharyngeal, prostate, and thyroid cancer; leukemia; melanoma; and multiple myeloma (see Table 1).
Occupational studies can also offer evidence of solar UVB’s effect on cancer risk. A recent study used cancer incidence data for 54 occupation categories based on 1.4 million male and 1.36 million female cancer cases for 1961–2005 in the five Nordic countries.23 The index for solar UVB irradiance used was incidence of lip cancer less incidence of lung cancer for males.7 The study used this index for both males and females because women wear lipstick, which reduces UVB irradiance on the lips. This index inversely correlated with both melanoma and nonmelanoma skin cancer (NMSC) for males. This finding is not surprising because sporadic UV
irradiance and chronic UVA irradiance are important risk factors for both melanoma and basal-cell carcinoma,24,25 whereas chronic sun exposure is not.26 This index significantly inversely correlated with 14 internal cancers (see Table 1); for women, the same UVB index was inversely correlated with bladder, breast, and colon cancer.7
UV irradiance is the primary risk factor for NMSC. Thus, diagnosis of or death from NMSC can sometimes serve as an index of high serum 25(OH) D concentration over a prolonged period. Two ecological studies inversely correlated internal cancer mortality rates with NMSC mortality rates: one in Spain for 1978–199227 and one in California for 1950–1964.28 A recordlinkage study also found significant inverse correlations between diagnosis of basal-cell carcinoma and squamous-cell carcinoma in sunny countries (Australia, Singapore, and Spain) and liver, lung, and pancreatic cancer, as well as nonsignificant inverse correlation with bladder, colon, gastric, ovarian, prostate, and renal cancer.8 Diagnosis of these skin cancers directly correlated with all types of cancer in less sunny countries. The likely explanation for the difference between the two types of countries is that sunnier countries are warm enough that people spend more time in the sun and expose more skin area when they do.
Researchers do not consider the ecological approach reliable in general because (1) the ecological approach does not deal with individuals and (2) confounding factors may explain the observed associations. However, for cancer, I find the ecological approach strong. In addition to consistent findings in many countries, other evidence exists that vitamin D reduces cancer risk, and researchers have proposed no mechanism other than vitamin D production to explain the findings of ecological studies. Hill’s criteria for causality in a biologic system offer a way to evaluate the UVB–vitamin D–cancer hypothesis.29 A recent conference in Germany recommended using Hill’s criteria as the basis for evidence-based nutrition.30 The criteria most important for UVB and vitamin D and cancer are strength of association, consistent findings in different populations, biologic gradient (dose–response relation), plausibility (e.g., mechanisms), experiment (e.g., RCTs), analogy, and accounting for confounding factors. These criteria have been examined for cancer in general and found largely satisfied for breast and colorectal cancer, with good evidence that other cancers do as well, including bladder, esophageal, gallbladder, gastric, ovarian, rectal, renal, and uterine corpus cancer, as well as Hodgkin’s and non-Hodgkin’s lymphoma.31 Examining Hill’s criteria for breast cancer, Mohr and colleagues point out that the process of evaluating
evidence for nutrients should be different from that for pharmaceutical drugs, which are evaluated on the tenets of evidence-based medicine.32 They also discussed deficient, adequate, and optimal intakes. Diseases are not deficiencies of pharmaceutical drugs, although many diseases are a consequence of vitamin D deficiency. Also, nearly every cell in the body has a vitamin D receptor. The active metabolite of vitamin D, 1,25-dihydroxyvitamin D (calcitriol), activates the vitamin D receptor and can regulate hundreds of genes.33 No receptors exist for pharmaceutical drugs unless they are specifically targeted.
A recent set of papers in Anti-Cancer Agents in Medical Chemistry reviewed evidence that vitamin D reduced risk for cancer, noting that disagreement remains over strength of the evidence of that assertion. Some studies found no or direct correlations between serum 25(OH)D concentrations and cancer incidence rates, and no strong RCTs have been reported showing that oral vitamin D reduces risk for cancer.34 I present further evidence supporting that hypothesis.
Case–control studies of serum 25(OH)D concentrations have consistently found strong inverse correlations with respect to breast cancer incidence.35 A case–control study found a highly significant inverse correlation between serum 25(OH)D concentration and prevalence of ovarian cancer.36 Although some concern exists that the disease state may affect serum 25(OH)D concentrations, this effect does not seem to be demonstrated for cancer. First, people who have cancer generally do not know so until diagnosis and thus would not change any habits related to vitamin D. Second, when odds ratios for breast or colorectal cancer are plotted versus years of follow-up, findings from case–control studies lie on the regression fit to all the data.37 Also, no studies have shown that cancer tumors reduce 25(OH)D concentrations. Organs afflicted with cancer can still synthesize calcitriol,38 but serum concentrations of calcitriol are about 1/1,000 those of 25(OH)D.
Prospective studies with follow-up times greater than 3 years have found nonsignificant inverse correlations between breast cancer incidence and 25(OH)D concentrations from serum drawn at time of enrollment.37 However, similar prospective studies of colorectal cancer have found significant inverse correlations for follow-up times as long as 12 years.37 The difference between these two cancers is that breast cancer grows much faster. For example, breast cancer diagnosis rates are higher in spring and fall. This finding has been attributed to vitamin D’s reducing risk in summer and melatonin in winter.39
A prospective study of seven cancers with respect to serum 25(OH)D concentration with a mean follow-up time of 9 years found no cancers with an inverse correlation with respect to serum 25(OH)D concentration.40 The problems with this study are not only the long follow-up time but also the few cancer cases. As a result, the 95 % confidence intervals for the odds ratio for the highest quantile of 25(OH)D were 30–50 %. See Grant41 for the relevance of number of cases.
Black Americans have lower cancer-specific and all-cause survival rates after diagnosis of cancer. Many studies have explored these relations, accounting for socioeconomic status, stage at diagnosis, and treatment provided, finding that blacks have survival rates anywhere from zero to 50 % lower than those of white Americans. Such studies were recently reviewed. The difference in population mean serum 25(OH)D concentrations for black Americans (16 ng/ml) and white Americans (26 ng/ml),42 along with the serum 25(OH)D–breast and colorectal cancer incidence relations,11 estimated the disparity in cancer survival rates at 25 %.43
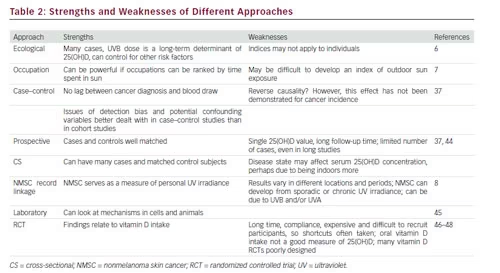
Table 1 summarizes evidence regarding the association of UVB and serum 25(OH)D concentration with respect to cancer incidence, prevalence, survival, or mortality rate. The table omits studies that found either no significant correlation or a direct correlation between UVB or serum 25(OH)D and cancer risk because they are thought to have systematic problems such as too few cases or unaccounted-for confounding factors. The strength of evidence is estimated by the number of types of studies supporting a beneficial role for each cancer. Nine cancers had what I judged to be strong evidence, eight had moderate evidence, and six had weak evidence. One problem with such ranking is that studying the less common cancers is harder because fewer cases are available.41 Most likely, several cancers with evidence ranked as moderate could be considered strongly affected by UVB and vitamin D. Table 2 gives an overview of strengths and weaknesses of various study types regarding vitamin D and risk for cancer.
Mechanisms
Studies have identified several mechanisms that explain how vitamin D reduces risk for cancer incidence and increases survival after cancer initiation. These effects are made by 1,25-dihydroxyvitamin D, generally by activating the vitamin D receptor. This active metabolite of vitamin D exerts several effects on cells, including controlling cellular proliferation and apoptosis. Vitamin D helps with calcium absorption, and calcium reduces risk for cancer.49 Vitamin D also reduces metastasis and angiogenesis around tumors. The literature includes several good reviews of vitamin D–cancer reduction mechanisms.50–52 The Garland group proposed a comprehensive model to explain how vitamin D reduces risk for cancer: “Its seven phases are disjunction, initiation, natural selection, overgrowth, metastasis, involution, and transition (abbreviated DINOMIT). Vitamin D metabolites prevent disjunction of cells and are beneficial in other phases”.50
Randomized Controlled Trials
Two vitamin D and calcium supplementation RCTs found reduced risk for cancer incidence. The first was conducted on postmenopausal women in Nebraska. They were divided into three arms: placebo, 1,450 mg of calcium per day, and 1,450 mg of calcium plus 1,100 IU of vitamin D3 per day.46 Between the ends of the first and fourth years, those taking calcium had a 41 % (95 % confidence interval [CI], −21 % to 71 %) reduced risk for all-cancer incidence, whereas those taking vitamin D plus calcium had a 77 % (95 % CI, 40 % to 91 %) reduction. Thus, a 36 % reduction occurred that could be attributed to vitamin D. In this study, that oral intake was associated with an increase in serum 25(OH)D concentration from 71.8 to 96.0 nmol/l. According to the graphical meta-analysis of the odds ratio of breast cancer incidence with respect to serum 25(OH)D concentration from case–control studies, the expected change in serum 25(OH)D concentration is 20 %. This value, which also has considerable uncertainty, generally agrees with the Nebraska results.
The second study was a reanalysis from the Women’s Health Initiative. This study considered only women who had not been taking personal vitamin D or calcium supplements before enrolling in the study. It reported the following: “In 15,646 women (43 %) who were not taking personal calcium or vitamin D supplements at randomization, CaD [calcium and vitamin D] significantly decreased the risk for total, breast, and invasive breast cancers by 14–20 % and nonsignificantly reduced the risk for colorectal cancer by 17 %. In women taking personal calcium or vitamin D supplements, CaD did not alter cancer risk (HR: 1.06–1.26)”.47 The general problem with vitamin D RCTs to date is that they have not been well designed. Lappe and Heaney48 outlined considerations for proper vitamin D RCTs:
- Start with an estimated serum 25(OH)D concentration–health outcome relation.
- Enroll people in the study who have serum 25(OH)D concentrations near the low end of the relation.
- Supplement them with enough vitamin D to raise serum 25(OH)D concentration to near the upper end of the relation.
- Consider other sources of vitamin D.
- Remeasure serum 25(OH)D concentrations during or at study end.
So few RCTs have followed these guidelines that when the Institute of Medicine reviewed the evidence that vitamin D reduced risk for adverse health outcomes, it found convincing evidence from RCTs only for bones.53
Another problem is that the time of life when vitamin D or diet is beneficial may be at a much younger age than that of those enrolled in RCTs, and determining whether younger people were used may take many years. Several studies found reduced risk for cancer for those with higher solar UVB irradiance in youth or early adulthood.59 A multicountry ecological study found that animal fat in the national dietary supply was highly correlated with rates for many cancers.55 This finding was disputed for nearly 3 decades until cohort studies found that animal products were an important risk factor for breast cancer for younger women.56 Studies of risk factors for Alzheimer’s disease should enroll people for 40 years.57
Ultraviolet Irradiance and Vitamin D Concerns
Because the strongest evidence that vitamin D reduces cancer risk comes from ecological studies based on indices of solar UVB doses, people could be advised to spend more time in the sun.58 Although doing so entails risk for skin cancer and melanoma, the risk should be minimal for those with skin type suited for the UV dose where they live.59 One should not stay in the sun long enough to develop erythema, or reddening.
Concerns have emerged about adverse health effects of serum 25(OH)D concentrations above 30 ng/ml, on the basis of finding U-shaped relations between serum 25(OH)D concentration and health outcome such as mortality rate.60 Some studies do not find statistically significantly increased risks at higher concentrations, whereas others are not consistent with most other studies on the same topic. A possible explanation for some of the findings is that study participants with higher serum 25(OH)D concentrations may have been diagnosed with a vitamin D–deficiency disease such as osteoporosis and advised by their physician to supplement with vitamin D. This was most likely the case for women in a US frailty study61 because men had an inverse correlation between serum 25(OH)D concentration and frailty status.62
Other Benefits of Vitamin D
Good observational evidence shows that higher serum 25(OH)D concentrations reduces risk for many adverse health outcomes, including all-cause mortality rate,63 cardiovascular disease,64,65 and type 2 diabetes mellitus.66
Recommendations
In light of the rapidly mounting evidence that serum 25(OH)D concentrations above 30–40 ng/ml are associated with better health outcomes,67–69 people should try to reach those levels through a combination of moderate solar UVB irradiance and vitamin D supplementation. Considerable variation exists in serum 25(OH) D concentration for any oral vitamin D intake,70 so people can either take 1,000–4,000 IU of vitamin D per day69–70 or have serum 25(OH) D concentration measured before starting to increase 25(OH)D concentrations, then again after several months. For reference, US mean population serum 25(OH)D concentrations in the early 2000s were 16 ng/ml for black Americans, 21 ng/ml for Hispanic Americans, and 26 ng/ml for white Americans.42 Thus, about two-thirds of Americans had suboptimal serum 25(OH)D concentrations then, and with the rising prevalence of obesity, the fraction is probably higher now. Serum 25(OH) D concentrations above 30–40 ng/ml confer many health benefits, along with virtually no substantiated health risks below 100 ng/ml. And vitamin D supplements are inexpensive. Therefore, implementing these recommendations makes good public-health sense.